

Cognitive Behavioral Therapy
Solving problems the cognitive-behavioral way, problem solving is another part of behavioral therapy..
Posted February 2, 2022 | Reviewed by Ekua Hagan
- What Is Cognitive Behavioral Therapy?
- Find a therapist who practices CBT
- Problem-solving is one technique used on the behavioral side of cognitive-behavioral therapy.
- The problem-solving technique is an iterative, five-step process that requires one to identify the problem and test different solutions.
- The technique differs from ad-hoc problem-solving in its suspension of judgment and evaluation of each solution.
As I have mentioned in previous posts, cognitive behavioral therapy is more than challenging negative, automatic thoughts. There is a whole behavioral piece of this therapy that focuses on what people do and how to change their actions to support their mental health. In this post, I’ll talk about the problem-solving technique from cognitive behavioral therapy and what makes it unique.
The problem-solving technique
While there are many different variations of this technique, I am going to describe the version I typically use, and which includes the main components of the technique:
The first step is to clearly define the problem. Sometimes, this includes answering a series of questions to make sure the problem is described in detail. Sometimes, the client is able to define the problem pretty clearly on their own. Sometimes, a discussion is needed to clearly outline the problem.
The next step is generating solutions without judgment. The "without judgment" part is crucial: Often when people are solving problems on their own, they will reject each potential solution as soon as they or someone else suggests it. This can lead to feeling helpless and also discarding solutions that would work.
The third step is evaluating the advantages and disadvantages of each solution. This is the step where judgment comes back.
Fourth, the client picks the most feasible solution that is most likely to work and they try it out.
The fifth step is evaluating whether the chosen solution worked, and if not, going back to step two or three to find another option. For step five, enough time has to pass for the solution to have made a difference.
This process is iterative, meaning the client and therapist always go back to the beginning to make sure the problem is resolved and if not, identify what needs to change.

Advantages of the problem-solving technique
The problem-solving technique might differ from ad hoc problem-solving in several ways. The most obvious is the suspension of judgment when coming up with solutions. We sometimes need to withhold judgment and see the solution (or problem) from a different perspective. Deliberately deciding not to judge solutions until later can help trigger that mindset change.
Another difference is the explicit evaluation of whether the solution worked. When people usually try to solve problems, they don’t go back and check whether the solution worked. It’s only if something goes very wrong that they try again. The problem-solving technique specifically includes evaluating the solution.
Lastly, the problem-solving technique starts with a specific definition of the problem instead of just jumping to solutions. To figure out where you are going, you have to know where you are.
One benefit of the cognitive behavioral therapy approach is the behavioral side. The behavioral part of therapy is a wide umbrella that includes problem-solving techniques among other techniques. Accessing multiple techniques means one is more likely to address the client’s main concern.

Salene M. W. Jones, Ph.D., is a clinical psychologist in Washington State.
- Find a Therapist
- Find a Treatment Center
- Find a Psychiatrist
- Find a Support Group
- Find Teletherapy
- United States
- Brooklyn, NY
- Chicago, IL
- Houston, TX
- Los Angeles, CA
- New York, NY
- Portland, OR
- San Diego, CA
- San Francisco, CA
- Seattle, WA
- Washington, DC
- Asperger's
- Bipolar Disorder
- Chronic Pain
- Eating Disorders
- Passive Aggression
- Personality
- Goal Setting
- Positive Psychology
- Stopping Smoking
- Low Sexual Desire
- Relationships
- Child Development
- Therapy Center NEW
- Diagnosis Dictionary
- Types of Therapy

Understanding what emotional intelligence looks like and the steps needed to improve it could light a path to a more emotionally adept world.
- Coronavirus Disease 2019
- Affective Forecasting
- Neuroscience
10 Best Problem-Solving Therapy Worksheets & Activities

Cognitive science tells us that we regularly face not only well-defined problems but, importantly, many that are ill defined (Eysenck & Keane, 2015).
Sometimes, we find ourselves unable to overcome our daily problems or the inevitable (though hopefully infrequent) life traumas we face.
Problem-Solving Therapy aims to reduce the incidence and impact of mental health disorders and improve wellbeing by helping clients face life’s difficulties (Dobson, 2011).
This article introduces Problem-Solving Therapy and offers techniques, activities, and worksheets that mental health professionals can use with clients.
Before you continue, we thought you might like to download our three Positive Psychology Exercises for free . These science-based exercises explore fundamental aspects of positive psychology, including strengths, values, and self-compassion, and will give you the tools to enhance the wellbeing of your clients, students, or employees.
This Article Contains:
What is problem-solving therapy, 14 steps for problem-solving therapy, 3 best interventions and techniques, 7 activities and worksheets for your session, fascinating books on the topic, resources from positivepsychology.com, a take-home message.
Problem-Solving Therapy assumes that mental disorders arise in response to ineffective or maladaptive coping. By adopting a more realistic and optimistic view of coping, individuals can understand the role of emotions and develop actions to reduce distress and maintain mental wellbeing (Nezu & Nezu, 2009).
“Problem-solving therapy (PST) is a psychosocial intervention, generally considered to be under a cognitive-behavioral umbrella” (Nezu, Nezu, & D’Zurilla, 2013, p. ix). It aims to encourage the client to cope better with day-to-day problems and traumatic events and reduce their impact on mental and physical wellbeing.
Clinical research, counseling, and health psychology have shown PST to be highly effective in clients of all ages, ranging from children to the elderly, across multiple clinical settings, including schizophrenia, stress, and anxiety disorders (Dobson, 2011).
Can it help with depression?
PST appears particularly helpful in treating clients with depression. A recent analysis of 30 studies found that PST was an effective treatment with a similar degree of success as other successful therapies targeting depression (Cuijpers, Wit, Kleiboer, Karyotaki, & Ebert, 2020).
Other studies confirm the value of PST and its effectiveness at treating depression in multiple age groups and its capacity to combine with other therapies, including drug treatments (Dobson, 2011).
The major concepts
Effective coping varies depending on the situation, and treatment typically focuses on improving the environment and reducing emotional distress (Dobson, 2011).
PST is based on two overlapping models:
Social problem-solving model
This model focuses on solving the problem “as it occurs in the natural social environment,” combined with a general coping strategy and a method of self-control (Dobson, 2011, p. 198).
The model includes three central concepts:
- Social problem-solving
- The problem
- The solution
The model is a “self-directed cognitive-behavioral process by which an individual, couple, or group attempts to identify or discover effective solutions for specific problems encountered in everyday living” (Dobson, 2011, p. 199).
Relational problem-solving model
The theory of PST is underpinned by a relational problem-solving model, whereby stress is viewed in terms of the relationships between three factors:
- Stressful life events
- Emotional distress and wellbeing
- Problem-solving coping
Therefore, when a significant adverse life event occurs, it may require “sweeping readjustments in a person’s life” (Dobson, 2011, p. 202).

- Enhance positive problem orientation
- Decrease negative orientation
- Foster ability to apply rational problem-solving skills
- Reduce the tendency to avoid problem-solving
- Minimize the tendency to be careless and impulsive
D’Zurilla’s and Nezu’s model includes (modified from Dobson, 2011):
- Initial structuring Establish a positive therapeutic relationship that encourages optimism and explains the PST approach.
- Assessment Formally and informally assess areas of stress in the client’s life and their problem-solving strengths and weaknesses.
- Obstacles to effective problem-solving Explore typically human challenges to problem-solving, such as multitasking and the negative impact of stress. Introduce tools that can help, such as making lists, visualization, and breaking complex problems down.
- Problem orientation – fostering self-efficacy Introduce the importance of a positive problem orientation, adopting tools, such as visualization, to promote self-efficacy.
- Problem orientation – recognizing problems Help clients recognize issues as they occur and use problem checklists to ‘normalize’ the experience.
- Problem orientation – seeing problems as challenges Encourage clients to break free of harmful and restricted ways of thinking while learning how to argue from another point of view.
- Problem orientation – use and control emotions Help clients understand the role of emotions in problem-solving, including using feelings to inform the process and managing disruptive emotions (such as cognitive reframing and relaxation exercises).
- Problem orientation – stop and think Teach clients how to reduce impulsive and avoidance tendencies (visualizing a stop sign or traffic light).
- Problem definition and formulation Encourage an understanding of the nature of problems and set realistic goals and objectives.
- Generation of alternatives Work with clients to help them recognize the wide range of potential solutions to each problem (for example, brainstorming).
- Decision-making Encourage better decision-making through an improved understanding of the consequences of decisions and the value and likelihood of different outcomes.
- Solution implementation and verification Foster the client’s ability to carry out a solution plan, monitor its outcome, evaluate its effectiveness, and use self-reinforcement to increase the chance of success.
- Guided practice Encourage the application of problem-solving skills across multiple domains and future stressful problems.
- Rapid problem-solving Teach clients how to apply problem-solving questions and guidelines quickly in any given situation.
Success in PST depends on the effectiveness of its implementation; using the right approach is crucial (Dobson, 2011).
Problem-solving therapy – Baycrest
The following interventions and techniques are helpful when implementing more effective problem-solving approaches in client’s lives.
First, it is essential to consider if PST is the best approach for the client, based on the problems they present.
Is PPT appropriate?
It is vital to consider whether PST is appropriate for the client’s situation. Therapists new to the approach may require additional guidance (Nezu et al., 2013).
Therapists should consider the following questions before beginning PST with a client (modified from Nezu et al., 2013):
- Has PST proven effective in the past for the problem? For example, research has shown success with depression, generalized anxiety, back pain, Alzheimer’s disease, cancer, and supporting caregivers (Nezu et al., 2013).
- Is PST acceptable to the client?
- Is the individual experiencing a significant mental or physical health problem?
All affirmative answers suggest that PST would be a helpful technique to apply in this instance.
Five problem-solving steps
The following five steps are valuable when working with clients to help them cope with and manage their environment (modified from Dobson, 2011).
Ask the client to consider the following points (forming the acronym ADAPT) when confronted by a problem:
- Attitude Aim to adopt a positive, optimistic attitude to the problem and problem-solving process.
- Define Obtain all required facts and details of potential obstacles to define the problem.
- Alternatives Identify various alternative solutions and actions to overcome the obstacle and achieve the problem-solving goal.
- Predict Predict each alternative’s positive and negative outcomes and choose the one most likely to achieve the goal and maximize the benefits.
- Try out Once selected, try out the solution and monitor its effectiveness while engaging in self-reinforcement.
If the client is not satisfied with their solution, they can return to step ‘A’ and find a more appropriate solution.

Download 3 Free Positive Psychology Exercises (PDF)
Enhance wellbeing with these free, science-based exercises that draw on the latest insights from positive psychology.
Download 3 Free Positive Psychology Tools Pack (PDF)
By filling out your name and email address below.
Positive self-statements
When dealing with clients facing negative self-beliefs, it can be helpful for them to use positive self-statements.
Use the following (or add new) self-statements to replace harmful, negative thinking (modified from Dobson, 2011):
- I can solve this problem; I’ve tackled similar ones before.
- I can cope with this.
- I just need to take a breath and relax.
- Once I start, it will be easier.
- It’s okay to look out for myself.
- I can get help if needed.
- Other people feel the same way I do.
- I’ll take one piece of the problem at a time.
- I can keep my fears in check.
- I don’t need to please everyone.

5 Worksheets and workbooks
Problem-solving self-monitoring form.
Answering the questions in the Problem-Solving Self-Monitoring Form provides the therapist with necessary information regarding the client’s overall and specific problem-solving approaches and reactions (Dobson, 2011).
Ask the client to complete the following:
- Describe the problem you are facing.
- What is your goal?
- What have you tried so far to solve the problem?
- What was the outcome?
Reactions to Stress
It can be helpful for the client to recognize their own experiences of stress. Do they react angrily, withdraw, or give up (Dobson, 2011)?
The Reactions to Stress worksheet can be given to the client as homework to capture stressful events and their reactions. By recording how they felt, behaved, and thought, they can recognize repeating patterns.
What Are Your Unique Triggers?
Helping clients capture triggers for their stressful reactions can encourage emotional regulation.
When clients can identify triggers that may lead to a negative response, they can stop the experience or slow down their emotional reaction (Dobson, 2011).
The What Are Your Unique Triggers ? worksheet helps the client identify their triggers (e.g., conflict, relationships, physical environment, etc.).
Problem-Solving worksheet
Imagining an existing or potential problem and working through how to resolve it can be a powerful exercise for the client.
Use the Problem-Solving worksheet to state a problem and goal and consider the obstacles in the way. Then explore options for achieving the goal, along with their pros and cons, to assess the best action plan.
Getting the Facts
Clients can become better equipped to tackle problems and choose the right course of action by recognizing facts versus assumptions and gathering all the necessary information (Dobson, 2011).
Use the Getting the Facts worksheet to answer the following questions clearly and unambiguously:
- Who is involved?
- What did or did not happen, and how did it bother you?
- Where did it happen?
- When did it happen?
- Why did it happen?
- How did you respond?
2 Helpful Group Activities
While therapists can use the worksheets above in group situations, the following two interventions work particularly well with more than one person.
Generating Alternative Solutions and Better Decision-Making
A group setting can provide an ideal opportunity to share a problem and identify potential solutions arising from multiple perspectives.
Use the Generating Alternative Solutions and Better Decision-Making worksheet and ask the client to explain the situation or problem to the group and the obstacles in the way.
Once the approaches are captured and reviewed, the individual can share their decision-making process with the group if they want further feedback.
Visualization
Visualization can be performed with individuals or in a group setting to help clients solve problems in multiple ways, including (Dobson, 2011):
- Clarifying the problem by looking at it from multiple perspectives
- Rehearsing a solution in the mind to improve and get more practice
- Visualizing a ‘safe place’ for relaxation, slowing down, and stress management
Guided imagery is particularly valuable for encouraging the group to take a ‘mental vacation’ and let go of stress.
Ask the group to begin with slow, deep breathing that fills the entire diaphragm. Then ask them to visualize a favorite scene (real or imagined) that makes them feel relaxed, perhaps beside a gently flowing river, a summer meadow, or at the beach.
The more the senses are engaged, the more real the experience. Ask the group to think about what they can hear, see, touch, smell, and even taste.
Encourage them to experience the situation as fully as possible, immersing themselves and enjoying their place of safety.
Such feelings of relaxation may be able to help clients fall asleep, relieve stress, and become more ready to solve problems.
We have included three of our favorite books on the subject of Problem-Solving Therapy below.
1. Problem-Solving Therapy: A Treatment Manual – Arthur Nezu, Christine Maguth Nezu, and Thomas D’Zurilla

This is an incredibly valuable book for anyone wishing to understand the principles and practice behind PST.
Written by the co-developers of PST, the manual provides powerful toolkits to overcome cognitive overload, emotional dysregulation, and the barriers to practical problem-solving.
Find the book on Amazon .
2. Emotion-Centered Problem-Solving Therapy: Treatment Guidelines – Arthur Nezu and Christine Maguth Nezu

Another, more recent, book from the creators of PST, this text includes important advances in neuroscience underpinning the role of emotion in behavioral treatment.
Along with clinical examples, the book also includes crucial toolkits that form part of a stepped model for the application of PST.
3. Handbook of Cognitive-Behavioral Therapies – Keith Dobson and David Dozois

This is the fourth edition of a hugely popular guide to Cognitive-Behavioral Therapies and includes a valuable and insightful section on Problem-Solving Therapy.
This is an important book for students and more experienced therapists wishing to form a high-level and in-depth understanding of the tools and techniques available to Cognitive-Behavioral Therapists.
For even more tools to help strengthen your clients’ problem-solving skills, check out the following free worksheets from our blog.
- Case Formulation Worksheet This worksheet presents a four-step framework to help therapists and their clients come to a shared understanding of the client’s presenting problem.
- Understanding Your Default Problem-Solving Approach This worksheet poses a series of questions helping clients reflect on their typical cognitive, emotional, and behavioral responses to problems.
- Social Problem Solving: Step by Step This worksheet presents a streamlined template to help clients define a problem, generate possible courses of action, and evaluate the effectiveness of an implemented solution.
If you’re looking for more science-based ways to help others enhance their wellbeing, check out this signature collection of 17 validated positive psychology tools for practitioners. Use them to help others flourish and thrive.

17 Top-Rated Positive Psychology Exercises for Practitioners
Expand your arsenal and impact with these 17 Positive Psychology Exercises [PDF] , scientifically designed to promote human flourishing, meaning, and wellbeing.
Created by Experts. 100% Science-based.
While we are born problem-solvers, facing an incredibly diverse set of challenges daily, we sometimes need support.
Problem-Solving Therapy aims to reduce stress and associated mental health disorders and improve wellbeing by improving our ability to cope. PST is valuable in diverse clinical settings, ranging from depression to schizophrenia, with research suggesting it as a highly effective treatment for teaching coping strategies and reducing emotional distress.
Many PST techniques are available to help improve clients’ positive outlook on obstacles while reducing avoidance of problem situations and the tendency to be careless and impulsive.
The PST model typically assesses the client’s strengths, weaknesses, and coping strategies when facing problems before encouraging a healthy experience of and relationship with problem-solving.
Why not use this article to explore the theory behind PST and try out some of our powerful tools and interventions with your clients to help them with their decision-making, coping, and problem-solving?
We hope you enjoyed reading this article. Don’t forget to download our three Positive Psychology Exercises for free .
- Cuijpers, P., Wit, L., Kleiboer, A., Karyotaki, E., & Ebert, D. (2020). Problem-solving therapy for adult depression: An updated meta-analysis. European P sychiatry , 48 (1), 27–37.
- Dobson, K. S. (2011). Handbook of cognitive-behavioral therapies (3rd ed.). Guilford Press.
- Dobson, K. S., & Dozois, D. J. A. (2021). Handbook of cognitive-behavioral therapies (4th ed.). Guilford Press.
- Eysenck, M. W., & Keane, M. T. (2015). Cognitive psychology: A student’s handbook . Psychology Press.
- Nezu, A. M., & Nezu, C. M. (2009). Problem-solving therapy DVD . Retrieved September 13, 2021, from https://www.apa.org/pubs/videos/4310852
- Nezu, A. M., & Nezu, C. M. (2018). Emotion-centered problem-solving therapy: Treatment guidelines. Springer.
- Nezu, A. M., Nezu, C. M., & D’Zurilla, T. J. (2013). Problem-solving therapy: A treatment manual . Springer.

Share this article:
Article feedback
What our readers think.

Thanks for your information given, it was helpful for me something new I learned
Let us know your thoughts Cancel reply
Your email address will not be published.
Save my name, email, and website in this browser for the next time I comment.
Related articles

The Empty Chair Technique: How It Can Help Your Clients
Resolving ‘unfinished business’ is often an essential part of counseling. If left unresolved, it can contribute to depression, anxiety, and mental ill-health while damaging existing [...]

29 Best Group Therapy Activities for Supporting Adults
As humans, we are social creatures with personal histories based on the various groups that make up our lives. Childhood begins with a family of [...]

47 Free Therapy Resources to Help Kick-Start Your New Practice
Setting up a private practice in psychotherapy brings several challenges, including a considerable investment of time and money. You can reduce risks early on by [...]
Read other articles by their category
- Body & Brain (48)
- Coaching & Application (57)
- Compassion (26)
- Counseling (51)
- Emotional Intelligence (24)
- Gratitude (18)
- Grief & Bereavement (21)
- Happiness & SWB (40)
- Meaning & Values (26)
- Meditation (20)
- Mindfulness (45)
- Motivation & Goals (45)
- Optimism & Mindset (34)
- Positive CBT (27)
- Positive Communication (20)
- Positive Education (47)
- Positive Emotions (32)
- Positive Leadership (16)
- Positive Psychology (33)
- Positive Workplace (36)
- Productivity (16)
- Relationships (49)
- Resilience & Coping (35)
- Self Awareness (21)
- Self Esteem (37)
- Strengths & Virtues (30)
- Stress & Burnout Prevention (34)
- Theory & Books (46)
- Therapy Exercises (37)
- Types of Therapy (64)
- Bipolar Disorder
- Therapy Center
- When To See a Therapist
- Types of Therapy
- Best Online Therapy
- Best Couples Therapy
- Best Family Therapy
- Managing Stress
- Sleep and Dreaming
- Understanding Emotions
- Self-Improvement
- Healthy Relationships
- Student Resources
- Personality Types
- Verywell Mind Insights
- 2023 Verywell Mind 25
- Mental Health in the Classroom
- Editorial Process
- Meet Our Review Board
- Crisis Support
What Is Cognitive Training and Does It Work?
Kendra Cherry, MS, is a psychosocial rehabilitation specialist, psychology educator, and author of the "Everything Psychology Book."
:max_bytes(150000):strip_icc():format(webp)/IMG_9791-89504ab694d54b66bbd72cb84ffb860e.jpg "problem solving cognitive training")
Cara Lustik is a fact-checker and copywriter.
:max_bytes(150000):strip_icc():format(webp)/Cara-Lustik-1000-77abe13cf6c14a34a58c2a0ffb7297da.jpg "problem solving cognitive training")
Getty Images
What Is Cognitive Training?
- Potential Benefits
- Effectiveness
Should You Try Brain Training?
How to improve brain fitness.
Cognitive training is an approach that seeks to sharpen or maintain brain functions through the use of regular mental activities. These mental activities are intended to help cognitive abilities such as working memory, executive function, and problem-solving abilities.
There is a long-standing notion that playing brain games, such as puzzles and memorization activities, can help stave off the negative effects of aging. But is the old "use it or lose it" adage really true? Do these cognitive games really have any sort of impact on mental functioning ?
This training may be beneficial for helping people to maintain and even improve some aspects of cognition. With a large population of aging adults, such improvements could have a significant impact on the mental health and functioning of older adults.
At a Glance
The goal of cognitive training is to sharpen the mind and help people hold on to their mental abilities as they age by playing games, solving jigsaw puzzles, or completing memory tasks. But does it really work? Researchers aren't 100% sure. Training improves skills on some tasks, but it's still uncertain if those results transfer to everyday life. However, there's certainly no harm in using cognitive training to stay engaged, focused, and mentally active.
So what can you do to boost your brain fitness? Learning to play an instrument, learning a new language, staying socially engaged, and getting regular exercise are just a few strategies that can help.
Also known as brain training, cognitive training is a non-pharmacological approach that involves following a series of regular mental activities designed to help maintain or even increase a person's cognitive (thinking) abilities.
Some of the mental abilities that are often targeted by cognitive training include:
- Cognitive flexibility
- Problem-solving
- Working memory
In addition to this specific brain training, there are also more general forms of mental training that can help retain or improve mental fitness and cognitive functioning. This more general mental training focuses on keeping the brain "fit," much the way exercise improves and maintains physical health.
General types of mental training can take a variety of forms, including physical exercise, playing video games, staying socially engaged, and participating in creative pursuits.
Potential Benefits of Cognitive Training
The focus of these activities is to help people become better at things like learning, solving problems, and reasoning. Some of these brain training activities focus on doing things like helping people remember more or improving their ability to focus and pay attention.
Such abilities have obvious uses in daily life. Being able to pay attention may help you focus on a class lecture or complete tasks without getting distracted. Being able to remember more might help you learn new things efficiently or recall the names of new people you meet.
Research has also found that these abilities are strongly linked to things such as intelligence , school achievement, and overall success in life.
Given the importance of these skills, it is perhaps not surprising that researchers have long been interested in knowing if such abilities are malleable.
Uses for Cognitive Training
There are a number of reasons why people might want to try cognitive training. These include:
- Slowing the cognitive declines associated with aging
- Helping older adults remain more independent
- Sharpening mental skills needed in daily life
Mental abilities that tend to decrease with age include processing speed, reaction time, decision making , short-term memory , and planning skills. Brain training may help sharpen these abilities, and it may help reduce the risks of some age-related memory problems.
One 2016 study, for example, found that training focused on improving processing speed reduced the risk for developing dementia a decade later.
There is also hope that some types of brain training may be useful for addressing certain types of impairments or problems. For example, in 2020, the FDA approved a brain training game designed to help treat attention deficit hyperactivity disorder (ADHD) .
The treatment is delivered via a video game that has been shown in several clinical trials to improve attention in children with ADHD. These effects also translated into meaningful improvement in daily functioning after a month of treatment. Such results show the potential that brain training may have.
Effectiveness of Cognitive Training
Researchers have been studying the impact of brain training for decades. However, there continues to be surprisingly little consensus on the effectiveness of cognitive training.
While there is research that supports the idea that specific brain training exercises can improve specific cognitive skills, there are other studies that have arrived at different conclusions.
Despite this lack of agreement in the research, an entire industry of apps, games, and other tools has emerged based on the idea that playing these brain games can improve your mental abilities.
Do Skills Transfer to the Real World?
And while there is some support for brain training, researchers have also questioned whether the skills gained during these training exercises transfer to real-world activities. In other words, does playing a memory training game really mean you'll remember what you needed to get at the grocery store?
There is some research that supports the use of brain training and its transferability to daily life and functioning. In one large-scale study, mental training was found to improve the cognitive function of older adults that led to lasting real-world improvements such as recalling when to take their medications.
The potential for such lasting benefits could help older adults maintain their mental abilities and independence as they age.
It's not just aging brains that stand to benefit from cognitive training. Research also suggests that brain training games can help improve executive functions such as working memory and processing speed in younger adults as well.
Why Results May Vary
The question, then, is why have some studies supported the positive effects of cognitive training while others have not found such effects? There may be a few factors at work.
- Not all types of brain training are equal: The broad nature of "cognitive training" itself means that different studies may not be looking at the same thing. The types of brain training used in research may lead to different effects both in lab settings and in how (and if) those skills might later be transferred into the real world.
- It may help some more than others : It is also important to note that much of the research does not account for individual differences. Memory training may be useful for people who are experiencing specific memory deficits, but people with normal abilities may experience less significant effects.
- It may have limited effects : One review of the research suggested that while brain training may be beneficial, it may be most effective for tasks that are very similar to the training activity. It also appears that this training may be more beneficial when it is done over an extended period of time.
If you are interested in using brain training, there are a few different things you can do. Cognitive training exercises often involve such things as pattern detection, using a touch screen program to increase thinking speed, and memorizing lists. Such activities can often be found online or by using mobile apps.
There are some things you should remember before trying these websites, games, or apps, however:
- Many brain training companies exaggerate the benefits of their products.
- Researchers have yet to uncover what elements make brain training interventions effective.
- Research has also not determined which types of training or what combination of training is needed to be effective for different conditions or problems.
- The types of apps and games that are available to consumers have usually not been scientifically tested to demonstrate their validity or effectiveness.
Some of these brain training companies were actually fined by the Federal Trade Commission (FTC) for making misleading claims about the benefits of their games.
A 2016 study compared the effects of the brain-training tool Lumosity to regular video games. The results found that both groups showed improvements in cognitive abilities—but so did other participants who didn't play any games at all.
The reality is that cognitive training may or may not work, but engaging in mentally stimulating activities is always a good thing.
Finding ways to challenge your brain may help you feel sharper now and protect your brain as you age.
If you want to try more general mental training designed to improve overall brain fitness, you might want to focus on doing mental exercises on your own. Some brain-boosting activities that might be helpful include:
- Do math in your head
- Draw a map from memory
- Learn a new language
- Learn how to play an instrument
- Memorize lists and test your recall
- Play Sudoku
- Put together a jigsaw puzzle
In addition to such cognitive training, there are other things that you can do to help take care of your brain. Activities that can improve your brain health include getting regular exercise , being socially active , and meditating .
Cognitive training may have a number of potential benefits, but it is also important to understand the limitations. It may sharpen your skills and help you retain more information, but you shouldn't expect miraculous improvements.
Such skills may or may not translate to the real world. If nothing else, these brain games can be a fun, challenging way to put your cognitive skills to the test.
Rather than focusing on training for a specific mental ability such as working memory, you might be better off focusing on things that promote long-term brain health and fitness. These include staying physically active, managing your stress , getting plenty of sleep, and maintaining social connections.
Yates LA, Ziser S, Spector A, Orrell M. Cognitive leisure activities and future risk of cognitive impairment and dementia: Systematic review and meta-analysis . International Psychogeriatrics . 2016;28(11):1791-1806. doi:10.1017/S1041610216001137
Katz B, Shah P, Meyer DE. How to play 20 questions with nature and lose: Reflections on 100 years of brain-training research . Proc Natl Acad Sci U S A . 2018;115(40):9897-9904. doi:10.1073/pnas.1617102114
Qiu C, Johansson G, Zhu F, Kivipelto M, Winblad B. Prevention of cognitive decline in old age-varying effects of interventions in different populations . Ann Transl Med . 2019;7(Suppl 3):S142. doi:10.21037/atm.2019.06.19
National Institute on Aging. Cognitive health in older adults .
Edwards JD, Xu H, Clark DO, Guey LT, Ross LA, Unverzagt FW. Speed of processing training results in lower risk of dementia . Alzheimer’s & Dementia: Translational Research & Clinical Interventions . 2017;3(4):603-611. doi:10.1016/j.trci.2017.09.002
U.S. Food & Drug Administration (FDA). FDA permits marketing of first game-based digital therapeutic to improve attention function in children with ADHD .
Kollins SH, DeLoss DJ, Cañadas E, et al. A novel digital intervention for actively reducing severity of paediatric ADHD (Stars-adhd): A randomised controlled trial . The Lancet Digital Health . 2020;2(4):e168-e178. doi:10.1016/S2589-7500(20)30017-0
Tennstedt SL, Unverzagt FW. The ACTIVE study: Study overview and major findings . J Aging Health . 2013;25(8 Suppl):3S-20S. doi:10.1177/0898264313518133
Nouchi R, Taki Y, Takeuchi H, et al. Brain training game boosts executive functions, working memory and processing speed in the young adults: A randomized controlled trial . PLoS ONE . 2013;8(2):e55518. doi:10.1371/journal.pone.0055518
Hampshire A, Sandrone S, Hellyer PJ. A large-scale, cross-sectional investigation into the efficacy of brain training . Front Hum Neurosci . 2019;13:221. doi:10.3389/fnhum.2019.00221
Federal Trade Commission (FTC). Lumosity to pay $2 million to settle FTC deceptive advertising charges for its "brain training" program .
Kable JW, Caulfield MK, Falcone M, et al. No effect of commercial cognitive training on brain activity, choice behavior, or cognitive performance . J Neurosci . 2017;37(31):7390-7402. doi:10.1523/JNEUROSCI.2832-16.2017
By Kendra Cherry, MSEd Kendra Cherry, MS, is a psychosocial rehabilitation specialist, psychology educator, and author of the "Everything Psychology Book."
- Bob Kauffman
- Testimonials
- Cognitive Behavioral Therapy
- Neurofeedback & Biofeedback
- Success Coaching
- Panic Attacks
- Concussions
- Brain Injuries
- Teens – Ages 13 to 18
- Teens – Ages 13 to 18 (Parent Version)
- Children – Ages 7 to 12
How Can Cognitive Training Improve my Problem-Solving Skills?

Learn How Cognitive Training Can Benefit Your Problem-Solving Abilities
The most striking quality about powerhouses like Bill Gates or Elon Musk is their extraordinary ability to innovate creative solutions. Admittedly it’s easy to feel like they’re somehow different from us—somehow more naturally inspired and resourceful than the average person. But believe it or not, you can also train your brain to think like a genius . In fact, you can accomplish amazing feats just by sharpening your problem-solving skills and learning to navigate challenges.
It all starts with cognitive training.
No matter who you are, your problem-solving abilities depend on the core cognitive skills you use every day. Cognitive training helps you hone those skills so you can accomplish more in the day-to-day of your professional life. Let’s take a closer look at those skills.

Cognitive training makes you better at solving problems alone or in a team.
How Does Problem-Solving Depend on Cognitive Skills?
Essentially, cognitive skills are the building blocks of all your thought processes. In fact, they’re used so frequently that most of the time you aren’t even aware of them—much like breathing. However, once you start noticing and actively working on them, you’ll become more capable and effective than ever.
Cognitive skills related to information-processing and problem-solving :
- Direction and Orientation: These skills make it easier to understand relationships in the environment. They allow you to give, take, and prioritize directions.
- Classification and Categorization: These skills allow you to group and reorganize ideas, emotions, objects, actions, and time periods. They help you deal with complicated tasks.
- Environmental Awareness: This is how well you see how different things are related. It helps you develop mental templates for dealing with similar situations.
- Analysis and Synthesis: These skills break down ideas and challenges into smaller, more manageable pieces. They keep you from becoming overwhelmed by too much information.
- Motor Integration: This skill makes it easier for you to set aside emotions and plan tasks out ahead of time.
- Concrete Sequencing: This skill makes you more aware of what is and isn’t working when carrying out a plan. It helps you to think logically and identify potential problems.
- Pattern Recognition: This skill helps you identify patterns and allows you to manage complicated or repetitive information.
How Will Cognitive Training Help?
Now, what can you do to develop those problem-solving skills and improve your on-the-job performance?
At Critical Thinking for Success, we start out by administering proficiency tests that identify which skills have the most room for growth . This lets us hone in on the skills that will benefit you the most. Once we’ve determined where to focus our efforts, we develop an individualized training regimen just for you . Furthermore, this training regimen involves daily exercises as well as in-person sessions.
Additionally, for each cognitive skill there are a variety of games, puzzles, and other exercises to help your development. For example, we use games and puzzles where moving one piece changes the rest of the board, forcing you to visualize a plan before you execute it rather jumping right into blind experimentation. This way, you train your brain to take an analytical approach and assess the inner logic and relationships behind a problem before you try to tackle it.
At our in-person sessions, we’ll review your progress with those exercises, as well as how you’ve been doing in your personal and professional life. We’ll discuss ways you can apply your cognitive training and suggest strategies for using them to face upcoming real-life challenges.
As you progress, you’ll see yourself having an easier time coming up with effective and creative solutions to the problems you face, and getting more done with less stress. That’ll make you more resourceful, more capable of handling whatever comes your way, and all-around a better business professional.
Ready to boost your problem-solving skills and take the next step toward accomplishing your dreams?
Call Critical Thinking for Success at 847-845-0422 . Let’s set up a consultation, and discuss how we can train your brain to be a problem-solving machine!
Author: Critical Thinking for Success
Related posts.


An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
Enhancing Cognitive Abilities with Comprehensive Training: A Large, Online, Randomized, Active-Controlled Trial
Joseph l. hardy.
1 Department of Research and Development, Lumos Labs, San Francisco, California, United States of America
Rolf A. Nelson
2 Department of Psychology, Wheaton College, Norton, Massachusetts, United States of America
Moriah E. Thomason
3 Merrill Palmer Skillman Institute for Child and Family Development, Wayne State University, Detroit, Michigan, United States of America
4 Department of Pediatrics, Wayne State University School of Medicine, Detroit, Michigan, United States of America
Daniel A. Sternberg
Kiefer katovich, faraz farzin, michael scanlon.
Conceived and designed the experiments: JLH FF RAN MET DAS MS. Performed the experiments: JLH FF DAS MS. Analyzed the data: DAS KK. Wrote the paper: JLH RAN MET DAS KK FF MS.
Associated Data
The study data for the statistical comparisons of outcomes for cognitive training relative to crosswords are in a CSV file in Supporting Information.
A variety of studies have demonstrated gains in cognitive ability following cognitive training interventions. However, other studies have not shown such gains, and questions remain regarding the efficacy of specific cognitive training interventions. Cognitive training research often involves programs made up of just one or a few exercises, targeting limited and specific cognitive endpoints. In addition, cognitive training studies typically involve small samples that may be insufficient for reliable measurement of change. Other studies have utilized training periods that were too short to generate reliable gains in cognitive performance.
The present study evaluated an online cognitive training program comprised of 49 exercises targeting a variety of cognitive capacities. The cognitive training program was compared to an active control condition in which participants completed crossword puzzles. All participants were recruited, trained, and tested online (N = 4,715 fully evaluable participants). Participants in both groups were instructed to complete one approximately 15-minute session at least 5 days per week for 10 weeks.
Participants randomly assigned to the treatment group improved significantly more on the primary outcome measure, an aggregate measure of neuropsychological performance, than did the active control group (Cohen’s d effect size = 0.255; 95% confidence interval = [0.198, 0.312]). Treatment participants showed greater improvements than controls on speed of processing, short-term memory, working memory, problem solving, and fluid reasoning assessments. Participants in the treatment group also showed greater improvements on self-reported measures of cognitive functioning, particularly on those items related to concentration compared to the control group (Cohen’s d = 0.249; 95% confidence interval = [0.191, 0.306]).
Taken together, these results indicate that a varied training program composed of a number of tasks targeted to different cognitive functions can show transfer to a wide range of untrained measures of cognitive performance.
Trial Registration
ClinicalTrials.gov NCT-02367898
Introduction
Recent evidence suggests that engaging in cognitively challenging activities can positively impact brain function, with studies demonstrating behavioral [ 1 , 2 ], physiological [ 3 , 4 ], and real-world functional [ 5 , 6 ] gains. This notion is supported by growing empirical evidence that neuroplasticity–the tendency for the nervous system to adapt to environmental challenges presented to it–is a fundamental principle of brain organization [ 7 – 9 ].
New appreciation of the importance of neuroplasticity has led to the development of a variety of cognitive training programs–activities designed to elicit enhancements in cognitive abilities through intensive, targeted mental exercise. Several such programs have been used in research, with promising results for improving cognitive functioning following training reported in most cases [ 2 , 4 , 10 – 16 ]; however, other studies have failed to demonstrate such gains [ 17 , 18 ]. Because cognitive abilities are critical for success at work [ 19 ], school [ 20 – 22 ], and activities of daily living [ 23 ], there is considerable interest in using large-scale approaches to rigorously investigate the efficacy of cognitive intervention strategies.
The present study enrolled participants via the Internet into either a cognitive training treatment condition or an active control condition. The treatment was the off-the-shelf version of Lumosity, an online cognitive training program, where participants trained on up to 49 tasks that were presented in game-like formats. Specific tasks within the program were designed to target particular cognitive abilities, such as speed of processing, working memory, divided attention, response inhibition, and fluid reasoning. Training tasks challenged users to operate close to their performance thresholds. A wide variety of tasks were used in training, reducing the opportunity for use of task-specific strategies. This variety increased the opportunity for “learning to learn,” which may enhance transfer to untrained tasks [ 24 ]. Previous studies using this program have demonstrated improvements in cognition in children with Turner’s Syndrome [ 25 ]; pediatric cancer survivors [ 26 ]; healthy middle-aged adults [ 27 ]; healthy older adults [ 28 ]; older adults with mild cognitive impairment [ 29 ]; and adult survivors of breast cancer [ 30 ].
The active control group in this study engaged in solving crossword puzzles. This activity was chosen because crossword puzzles constitute a challenging mental activity that is popularly believed to be beneficial for cognition [ 31 ]. Some health professionals specifically advocate the use of crossword puzzles for sharpening mental skills [ 32 ]. While there is relatively little experimental evidence supporting the efficacy of crossword puzzles, one observational study has linked regular engagement with crossword puzzles to a delay in the onset of memory decline in older adults [ 33 ].
The goal of this study was to measure the efficacy of a targeted, progressively challenging, comprehensive cognitive training program against a plausibly beneficial active control condition in a large, randomized trial. We hypothesized that this type of cognitive training would show greater transfer to a range of underlying cognitive abilities than the active control, as measured by a broad battery of neuropsychological assessments and participant-reported outcomes.
Ethics statement
Participants provided informed consent by clicking a dialogue box on a digital consent form prior to participation in the study. All study materials and procedures were approved by an independent institutional review board (Ethical and Independent Review Services; Corte Madera, CA). The IRB-approved study protocol is included as Supporting Information ( S1 Protocol ).
Trial registration
The study was registered on ClinicalTrials.gov (NCT-02367898) upon the request of the journal staff. The investigators had not previously registered on the site, as the trial did not involve a clinical population. The authors confirm that all ongoing and related trials for this intervention are now registered.
Participants
Participants were recruited from the Lumosity website ( www.lumosity.com ). Individuals who had created an account on the site, but who were not paying subscribers (i.e., free users) were eligible for recruitment. Invitations were sent via email to users who engaged with the program on at least three days in the first week after sign-up. All participants who completed the study were compensated with a 6-month membership to Lumosity.
A power analysis based on results from an open-label study of the treatment program, a portion of which has been presented previously [ 34 ], suggested that 5,000 participants (2,500 per group) would provide greater than 99% power to obtain significance on the primary outcome measure and greater than 70% to detect a dose-response interaction between groups, if one existed. Based on the ongoing study completion rate, recruitment ended when it was estimated that the number of participants enrolled in the study would be sufficient to obtain 5,000 fully evaluable participants.
In total, 11,470 individuals consented to take part in the study and completed a baseline (pre-test) assessment battery. The first participant was randomized on April 27, 2013, and the final participant completed the post-test on April 28, 2014. Participants were assigned a treatment condition using a random number generator with equal probabilities of assignment to cognitive training and crosswords control conditions. Random assignment occurred after the pre-test. Participants with age falling outside the target range of 18–80 were excluded prior to randomization (N = 1,272). An additional 279 participants were excluded because a computer error delayed their randomization into a treatment condition by more than 24 hours, allowing these participants to continue with the Lumosity program in the free user state. Of the remaining 9,919 participants randomized into a treatment condition, 5,045 (50.9%) completed the post-study assessment battery (post-test). The training platform was designed to direct each participant, upon logging in each day, to either cognitive training or crossword puzzles based on his or her group assignment. However, in some cases participants in the crossword control group were able to access cognitive training. As a result, 330 control participants were removed from the primary analysis because they accessed the cognitive training program during the study period ( Fig 1 ). See Table 1 for demographic characteristics of the fully evaluable cohorts in both conditions. Age, gender, and educational attainment were evenly distributed across the groups.

P values are based on Kolmogorov-Smirnov test for age, chi-square for gender and education. Statistics for gender and education are based on participants who reported this information.
Treatment and control groups
All participants were instructed to log into the website and do one session per day of their activity (cognitive training for the treatment group or crossword puzzles for the control group), 5 days a week for 10 weeks. Daily email participation reminders were sent to all participants during the study period.
Cognitive training treatment
The Lumosity cognitive training program was used as the treatment condition in this study. Treatment participants in this study received the same training experience that Lumosity subscribers received over the same period of time. Daily training sessions included five cognitive training tasks. On any given day, the five tasks for that particular session were chosen by an algorithm that attempted to optimize a balance of training activities such that tasks were presented in clusters across days without repeating individual tasks on a given day. One five-task session typically took approximately 15 minutes to complete. Outside of this session, participants could opt to do additional training with any of the 49 available tasks in an a la carte fashion.
The cognitive training tasks each target a particular core cognitive ability and are grouped into five categories by target domain: speed of processing, attention, memory, flexibility, and problem solving. Many of these tasks are described in detail elsewhere in the literature [ 25 – 27 , 29 , 30 , 35 – 37 ], and a description of all tasks is included as Supporting Information ( S1 Appendix ).
Crossword puzzles control
Participants randomized into the active control group received a daily session timed at a minimum of 15 minutes. They were instructed to complete as many crossword puzzles as possible in the allotted time. If a participant completed a puzzle within the 15-minute time period, the crossword application would provide a new puzzle. At the end of the 15-minute period, participants were able to continue to work on the current puzzle for as long as they chose but were not given additional puzzles that day. The crossword puzzles were produced by professional crossword constructors and presented in a web-based crosswords platform. Constructors were asked to create crosswords that were of medium difficulty, approximately equivalent to a Thursday New York Times crossword puzzle (note: the New York Times puzzles increase in difficulty throughout the week, culminating with the most difficult puzzle on Saturday). Participants filled out the puzzles by typing the answers in the appropriate boxes. Feedback about correct and incorrect responses was given immediately following submission of a completed crossword. The puzzles were placed in a website frame that replicated the look and feel of the cognitive training website in order match as closely as possible the experience across the two conditions.
Compliance with the study protocol was assessed via two measures: (1) the number of unique days that treatment participants completed at least one training task or control participants started a crossword puzzle (“active days”), and (2) the estimated total time participants spent engaging with the respective condition. See the Supporting Information ( S1 File ) for additional details on how engagement time was estimated. As participants were instructed and reminded to complete daily sessions, the number of active days was used as the primary measure of a participant’s ongoing engagement and compliance with the study protocol. Secondary analyses based on total time are included in S1 File .
Outcome measures
Outcomes were assessed using a battery of seven neuropsychological tests, as well as a participant-reported outcomes survey. The primary outcome measure used in this study was change in aggregate cognitive performance, as measured by the Grand Index (described further below) of the neuropsychological assessment battery, from before to after the 10-week study period. Secondary outcome measures included change in performance on each of the subtests in the neuropsychological battery and changes in responses to the survey. The assessments and survey were administered online in a pre-test one day prior to beginning the treatment or control condition. Participants were directed to take the post-test 70 days later, one day following the end of the treatment or control.
Neuropsychological assessment battery
Seven neuropsychological assessments were used in this study. (1) Forward and (2) Reverse Memory Span assessed visual short-term and working memory, respectively, and are based on the Corsi Blocks tasks [ 38 ]. These assessments required participants to recall a sequence of randomized spatial locations in either forward or reverse order. (3) Grammatical Reasoning was based on Baddeley’s Grammatical Reasoning Test [ 39 ], designed to assess cognitive flexibility and reasoning, and required participants to rapidly and accurately evaluate potentially confusing grammatical statements. (4) Progressive Matrices was based on established matrix reasoning assessments [ 40 ] and was designed to assess problem solving and fluid reasoning. (5) Go/No-Go was designed to assess response inhibition and processing speed, and required participants to respond as quickly as possible to a target stimulus while avoiding responding to distractors. (6) Arithmetic Reasoning was designed to assess numerical problem solving ability and required the participant to respond as quickly and accurately as possible to arithmetic problems written in words (e.g., “Four plus two =”) [ 41 ]. (7) Two-Target Search was created for the purposes of this study. This task was designed to measure divided visual attention and required participants to recall the locations of briefly presented target letters while ignoring distractors. See the Supporting Information ( S2 Appendix ) for more detailed information about the design of these assessments. Importantly, none of the tasks used in the outcome assessment battery were presented during training. Rather, outcome assessments were implemented as measures of transfer to underlying cognitive abilities.
Assessment scaling procedure
Our assessment scaling procedure follows standard rank-based normalization approaches used in well-established IQ tests [ 42 , 43 ]. Normalization tables were created based on the pre-test data from participants who completed both the pre- and post-tests, including control participants who completed some amount of cognitive training during the study period. Norms were generated in 5-year age bins and tables were created within each age bin for each assessment. These normalization tables were created by taking the empirically observed percentile rank for each raw score and finding the value corresponding to that percentile from a normal distribution with a mean of 100 and standard deviation of 15 (i.e., percentile rank normalization). For the Two-Target Search and Go/No-Go assessments, where the relevant raw score was presentation time or reaction time, raw scores were reverse coded before being subjected to the normalization procedure. The resulting normalized scores compared a participant’s score to all other participants within his or her age bin, with higher scores corresponding to better performance on that assessment. The Grand Index score was calculated based on the sum of a participant’s normalized scores on all assessments. This sum was then transformed using the same percentile rank normalization procedure described above.
Participant-reported outcomes
Participants also completed a survey including nine questions related to specific cognitive failures [ 44 ] and successes as well as emotional status. Participants took the survey immediately after completing the neuropsychological test battery, once before beginning the study period (pre-test) and once upon completion of the study (post-test).
The survey included four questions related to a participant’s self-reported cognitive performance over the past month and an additional five questions related to a participant’s cognitive performance and emotional status over the past week. Responses to the first group of four questions rated frequency of cognitive ability or impairment, whereas the second group of five questions rated agreement or disagreement with statements about participants’ cognition or emotion. (Note: some participants were also given an additional question regarding whether they “felt benefits from cognitive training”. Because this question did not apply equally to the treatment and control groups, and was not included in the original protocol, it was removed from the analysis. For completeness, responses to this question are included along with the rest of the study data in the attached S1 Dataset ). Response options for the first group of questions were: “Never”, “1–2 times during the month”, “1–2 times per week”, “Several times per week”, “Almost every day”, or “N/A”. Response options for the second group of questions were on a Likert scale: “Strongly disagree”, “Disagree”, “Neither agree nor disagree”, “Agree”, “Strongly agree”, or “N/A”. The survey items are presented in the Results section.
Primary outcome measure
Our primary hypothesis was that the treatment program would lead to greater improvements in aggregate cognitive performance compared to the active control, as measured by the neuropsychological assessment battery. If this hypothesis were correct, we would expect to see larger improvements from pre-test to post-test on the Grand Index of the assessment battery for the treatment group relative to the control group. Such differences in change scores were observed. The mean increase on the Grand Index score (post-pre) in the treatment group was 5.24 points (sd = 12.00), and the mean increase in the control group was 2.09 points (sd = 10.66) ( Fig 2 ). The 95% confidence interval for the mean difference of 3.15 points was 2.49 to 3.81.

Error bars represent confidence intervals bootstrapped over 100,000 iterations. Mean change scores and error bars are based on unadjusted summary statistics. P value is based on results from the ANCOVA analysis described in Table 2 . ***p < 0.001.
The difference in composite (Grand Index) change scores between the two groups (treatment vs. control) was evaluated with an ANCOVA model measuring the effect of group, controlling for the pre-test score. Pre-test score was included as a covariate to control for regression to the mean effects as well as any effects of baseline performance. Cohen’s d effect sizes were calculated using model-adjusted means and standard deviations throughout the following analyses [ 45 ]. The ANCOVA revealed that aggregate cognitive performance improvement in the treatment group was significantly greater than in the control group (t(4712) = 8.73, p < 10 −15 , Cohen’s d = 0.255, 95% confidence interval = [0.198, 0.312]) ( Table 2 ). While the improvement in the crosswords control group was also significant on a within-group basis (p < 10 −15 ), the treatment group improved more than twice as much as the control. The effect size of the within-group change score was d = 0.467 for the treatment group and d = 0.212 for the controls. These results indicate that the cognitive training treatment condition was more effective than the crosswords control for improving cognitive performance on the assessment battery on an aggregate basis.
Means and standard deviations of baseline and change scores are the unadjusted summary statistics. Significance levels and effect sizes are based on ANCOVA models controlling for pre-test means. For all analyses, N control = 2,048, N treatment = 2,667.
The model also revealed a significant negative effect of pre-test score (t(4712)) = -24.4, p < 10 −15 ), indicating that, on average, participants with lower pre-test scores showed greater improvements at post-test than those with higher pre-test scores. This effect may be due to a regression-to-the-mean effect and/or an effect of starting level.
To ensure that the exclusion of control participants who did some cognitive training with the treatment program (see Participants section in Methods ) could not explain these results, we performed an additional set of ANCOVA analyses ( S1 File ). These analyses repeated the ANCOVA approach described above, adding back in the participants from the control condition who were initially excluded because they performed some cognitive training during the study period (N = 330). The pattern of results and conclusions remained consistent across all comparisons (see S1 File ), indicating that these exclusions could not explain the main result that cognitive training led to larger gains in cognitive performance compared to crosswords.
In the primary analysis conducted here, no outliers were removed. All completed assessments were included in the analysis. In order to ensure that outliers did not play an important role in the findings, we completed a secondary outlier analysis (see S1 File ). In this analysis, any raw scores that were outside the range of three standard deviations above or below the mean were removed prior to further statistical analysis. The conclusions remained the same across all subtests included in the battery. The Grand Index change score analysis was recalculated for participants with no outliers. The between-group effect size for participants without outliers was Cohen’s d = 0.267 (95% confidence interval [0.208,0.326]). Based on this analysis, outlier effects could not account for the results of this study.
Individual assessments
Based on the significant main effect on our primary outcome measure, we performed secondary analyses consisting of additional ANCOVA models for each assessment. The models revealed that the cognitive training treatment group improved significantly more than the crossword puzzles control group on five of the seven assessments. Specifically, significantly larger improvements for the treatment relative to the control group were found for Forward and Reverse Memory Span, Progressive Matrices, Go/No Go, and Arithmetic Reasoning, while the control group improved more than the treatment group on Grammatical Reasoning. There was no statistically significant difference between the groups for the Two-Target Search task. Fig 3 provides an illustration of the unadjusted change scores for each assessment for both groups. ANCOVA model p values and effect sizes along with unadjusted pre-test means and change scores for each assessment are shown in Table 2 .

Error bars represent confidence intervals bootstrapped over 100,000 iterations. Mean change scores and error bars are based on unadjusted summary statistics. P values are based on results from the ANCOVA analyses listed in Table 2 . **p < 0.01, ***p < 0.001.
Effects of amount of engagement
If the cognitive training treatment was more effective than playing crossword puzzles for improving cognitive abilities, we may observe a larger effect of active days of study engagement for the treatment condition compared to the control condition. The distributions of number of active days were similar for the two training conditions (treatment: mean = 46.6, sd = 15.2, median = 50; control: mean = 45.5, sd = 19.6, median = 52). Participants in the crosswords condition were active on slightly fewer days than those in the treatment condition on average (t(4713) = 2.18, p = 0.030). In order to test for a group difference in the effect of active days, we constructed a general linear model predicting Grand Index change score from pre-test score, treatment group, active days, and the group-by-active-days interaction. The model revealed both a main effect of active days (B = 0.054, t(4710) = 4.47, p < 10 −5 ) and a group-by-active-days interaction (B = 0.043, t(4710) = 2.38, p = 0.017), indicating significant dose-response effects for both groups, with a significantly larger effect of dose for the cognitive training treatment group relative to controls ( Fig 4 ).

Lines represent estimates from the general linear model including effects of group, active day, and the group-by-active-days interaction. Shading represents 95% confidence intervals.
The estimated total time participants engaged with their respective conditions provides an additional measure of compliance. Total engagement time was similar across the two groups (treatment: mean = 16.1 hrs, sd = 16.4 hrs, median = 12.2 hrs; control: mean = 13.0 hrs, sd = 7.6 hrs, median = 13.6 hrs), with mean total engagement time being higher in the treatment condition and median total engagement time being higher in the control condition. These results indicate that participants in both conditions on average complied with the instructions to engage for at least 15 minutes per day, 5 days per week for 10 weeks (12.5 hrs total). See S1 File for matched sample analyses demonstrating that the observed group differences in overall cognitive performance improvement are not explained by differences in the distributions of total engagement time.
Of the 4,715 participants included in the analyses above, 4,697 (99.8%) also completed the participant-reported outcomes survey both before and after the study period. In order to calculate change scores on the survey, participant responses were first numerically coded on a scale from 0 to 4, with the scale always ranging from 0 as the most negative response to 4 as the most positive response. Responses to questions 1, 2, 3, 7, 8, and 9 were reverse coded to maintain consistency of response coding across all questions (i.e., such that a higher number indicated a more positive response). An average of the scores was taken for both pre- and post-tests as an overall measure of self-reported real-world cognitive performance and emotional status. The differences between pre- and post-test overall scores and scores on each question were analyzed.
The hypothesis that participants in the treatment group would show greater self-reported improvements in cognition and emotional status relative to control participants was tested via an ANCOVA model measuring the effect of group (treatment vs. control) on the change in average survey score, controlling for average pre-test score. The model revealed a main effect of group on change score, indicating that cognitive training resulted in larger increases in self-reported cognition and emotional status scores compared to the crossword puzzles control (t(4689) = 8.50, p < 10 −15 , Cohen’s d = 0.249, 95% confidence interval = [0.191, 0.306]). The improvement in the crosswords control group was also significant on a within-group basis (p < 10 −15 ). These results indicate that, overall, the cognitive training treatment was more effective than the crosswords control for improving self-reported real-world cognition and emotional status. Pre-test score was a significant negative predictor of post-test score (t(4689) = -39.8, p < 10 −15 ), indicating regression to the mean and/or effect of starting level.
For all nine questions, both groups tended to report improvements following study participation, compared to the pre-test. The changes were significant for both groups on all questions except for question 4 (memory for a new name). Results for each question are presented in Table 3 . Participants in the treatment group reported significantly larger improvements for eight of the nine questions compared to the control group (all ps<0.01). The three largest group differences were on questions 1, 3 and 6, all of which were related to concentration.
Means for questions 1, 2, 3, 7, 8 and 9 were reversed coded, such that higher scores should be interpreted as more positive responses for all questions. Means and standard deviations of baseline and change scores are the unadjusted summary statistics. Significance levels and effect sizes are based on ANCOVA models controlling for pre-test means. Degrees of freedom are based on participants giving non-“NA” answers at both time points.
The findings of this study are consistent with the extant literature on cognitive training that shows that progressively challenging, targeted cognitive training can be an effective tool for improving core cognitive abilities including speed of processing [ 13 ], working memory [ 46 ], and fluid reasoning [ 10 ]. The results presented here extend previous findings by demonstrating that a cognitive training program targeting a variety of cognitive capacities with different exercises can be more effective than crossword puzzles at improving a broad range of cognitive abilities.
After 10 weeks of training, participants receiving the cognitive training treatment improved more than those receiving crossword puzzles on Forward and Reverse Memory Span (measures of visual short term and working memory, respectively), Progressive Matrices (a measure of fluid reasoning), Go/No-Go (a measure of response inhibition and speed of processing), and Arithmetic Reasoning (a measure of problem solving). In addition, improvement on the overall measure of cognitive function used as the primary outcome measure in this study–the Grand Index for the assessment battery–was more than twice as large in the cognitive training group as it was in the crossword puzzles control group. Thus, for improving a variety of core cognitive abilities, the treatment used in this trial was more effective than crossword puzzles.
The Cohen’s d effect size for the between-group differences in the primary outcome measure (the Grand Index) was 0.255. Another approach to appreciating the magnitude of these results is to contextualize them in the distribution of scores on the outcome measures. We observe that participants in the training group improve by 2.77 points more than those in the crosswords group, after correcting for the pre-test score in our ANCOVA model. Given that the scores are scaled on a 100 mean ± 15 sd scale, we can evaluate how far an average participant would move within the population distribution (for their age) based on moving a given number of points. In this case, 2.77 points is the equivalent of moving from the 50 th percentile of the distribution to the 57 th percentile. This is a potentially meaningful move within the distribution.
A significant group-by-active-days interaction was observed in this study, such that an additional active day engaging with the cognitive training intervention was related to larger gains on the cognitive battery composite score compared to an additional active day engaging with crossword puzzles ( Fig 4 ). This suggests that additional training could lead to larger gains. While it is unlikely that the linear relation holds indefinitely (i.e., the function likely decelerates at some point), future work will be necessary to ascertain how much total improvement is possible over longer training periods.
In addition to the enhanced performance observed in the cognitive training group on the neuropsychological measures of cognitive function, participants in this group also self-reported experiencing benefits that were significantly greater than those reported by participants in the active control. These participant-reported improvements were particularly strong on questions related to the ability to concentrate. These results suggest that participants in the treatment group experienced benefits from the training in their everyday lives.
Crossword puzzles were chosen as the active control because they are commonly believed to be a cognitively stimulating activity that is good for brain health [ 31 , 32 ]. This is important because it has been suggested that belief in the efficacy of a training intervention could affect effort and performance on testing outcomes [ 47 ].
While not as large as the gains seen in the treatment group, participants in the crosswords control group also showed improvements in cognitive performance. Without a no-contact control group in this study, it is not possible to conclusively determine whether these improvements in the active control condition were due to practice effects, placebo effects, real treatment effects, or some combination of these. Further study will be needed to better understand the benefits of crossword puzzles for maintenance and enhancement of cognition. It is worth noting that participants in the crosswords group improved slightly more than the cognitive training group on a measure of grammatical reasoning. It would not be unreasonable to imagine that intense, concerted word finding training might enhance one’s performance on a linguistic task.
There are several reasons why the treatment program might have outperformed crossword puzzles in enhancing cognitive function. First, the cognitive training program is specifically targeted to core cognitive functions. This distinguishes the treatment from crossword puzzles, which are not designed with the goal of cognitive enhancement. Another central feature of the cognitive training program studied here is that it is progressively challenging –that is, many of the tasks explicitly increase in difficulty as the individual improves, while others encourage the individual to perform at threshold by rewarding increasingly faster and more accurate performance (see S1 Appendix ). This follows a long-established tenet in the psychological literature, that learning conditions are optimized when the task is challenging, but not prohibitively difficult [ 48 , 49 ]. Task variety and novelty are also potentially important. In the case of crossword puzzles, participants are primarily involved in vocabulary retrieval, challenging a more limited set of neural pathways. In the cognitive training program studied here, participants are challenged to engage with a variety of cognitive tasks that challenge different neural processing systems and do so in different ways. This variety limits the opportunity to solve the tasks with a single task-specific strategy, thus encouraging the learning of new strategies and the development of new neural connections.
We noted that there have been several studies that have reported not finding benefits from cognitive training. The only other similarly powered study that did not find positive results is a 2010 study that recruited 11,430 participants through a BBC television show and collected data online [ 17 ]. The authors concluded that brain training had no measureable benefits. Several key aspects of that study differ from the one presented here. First, neither of the two treatment conditions they used had been studied empirically prior to that experiment. As we demonstrate in this study, not all cognitively stimulating activities are equally effective for enhancing cognition, and it is possible that other programs not examined in their study are more effective. Also, the average amount of training exposure in the BBC study was less than half of that in this study. This is an important distinction as results of this study indicate that amount of training is related to the magnitude of gains in cognitive performance ( Fig 4 ).
Our results represent statistically significant improvements in cognitive processes through training. This study included a sufficiently large number of participants and enough training to reliably detect these effects. As has been noted previously [ 50 ], most cognitive training studies that have shown null results have not been powered in such a way that either a positive or a null outcome would be informative, and often include quite short training periods. In the broader context of factors influencing cognitive processes (i.e., a lifetime of experiences), even the 10 weeks of training in this study is a fairly modest amount. Further research will be needed to understand how the current effects extrapolate over much longer training periods.
In this study, 49.1% of participants randomized into one of the two conditions were lost to follow-up (i.e., did not take the post-test). There was little difference in dropout rates between the two groups, and supplemental analyses ( S1 File ) that equated the engagement characteristics of completers from both groups demonstrated that these differences in dropout between the two groups could not explain the results.
This study utilized an entirely online design. The online methodology is ecologically valid, since most users in the real world experience the program at home or in some other personal environment outside a laboratory or clinic. In traditional laboratory-based training studies, participants experience considerable contact with study personnel. Contact with study personnel may lead to lower rates of loss to follow up. However, this personal interaction introduces a variable that could affect the results and is not reflective of how most normal, healthy adults use these programs.
A possible limitation of the current study is that it does not isolate specific mechanisms. For example, adaptive difficulty may play an important role in driving the transfer of training [ 51 ]. Many of the tasks in the cognitive training program were explicitly adaptive (i.e., difficulty was increased as performance improved), whereas the crossword puzzles were not. The two conditions differed on other dimensions as well. The cognitive training program incorporated a variety of tasks that targeted specific cognitive functions, while the crosswords condition did not. Future research is needed to more fully elucidate the relative contributions of particular components of activities that lead to improvements in cognitive performance.
Future studies could also extend the cognitive domains tested. Our neuropsychological assessment battery was relatively comprehensive across a variety of domains, but not every possible dimension of cognition was addressed. For example, this battery did not include any assessment explicitly targeting learning (e.g., Hopkins Verbal Learning Test) or complex working memory (e.g., Counting Span).
Research on training to improve cognitive skills is not complete, and there remain many open questions. The ability to efficiently collect large data sets in controlled experiments over the Internet may prove crucial to answering the open questions related to cognitive training in the future.
Supporting Information
S1 consort checklist, s1 appendix, s2 appendix.
The first supplementary analysis is an ANCOVA analysis that includes participants assigned to the control group who engaged in some cognitive training during the study period. The second supplementary analysis describes how engagement time is estimated in the two conditions and provides a paired-matching analysis that controls for the total time spent engaging with the two conditions. The third supplementary analysis includes an outlier removal procedure.
S1 Protocol
Acknowledgments.
We would like to acknowledge the efforts of all the dedicated people who have worked to create Lumosity. We would like to thank Kacey Ballard Corrado and Tyler Hinman for their work to facilitate the creation of the crossword puzzles system that was used as the control condition. We would also like to thank Sylvia Bunge, Murali Doraiswamy, Jerri Edwards, Amit Etkin, Anett Gyurak, Christine Hooker, Joseph Ventura, and Mike Walker for their thoughtful comments on the manuscript.
Funding Statement
No external funding contributed to this research; Lumos Labs, Inc. funded the research through the development of its software tools and through the employment of JLH, DAS, KK, FF and MS and through the consulting services of RAN. The specific roles of these authors are articulated in the “Author Contributions” section. Other members of the company contributed suggestions and ideas during the design of the study and preparation of the manuscript, and provided support and advice to the authors during the process of submitting the manuscript for publication. Lumos Labs had no other role in the study design, data collection and analysis, decision to publish, and preparation of the manuscript. Legal approval for publication before submission of the manuscript was obtained from Lumos Labs.
Data Availability

Encyclopedia of Gerontology and Population Aging pp 1–7 Cite as
Cognitive Training
- Jerri D. Edwards 3
- Living reference work entry
- First Online: 01 July 2019
73 Accesses
Cognitive intervention
Cognitive training is targeted intervention aimed at improving specific mental abilities such as memory, attention, speed of processing, or executive function. Two major types of cognitive training are process-based, which includes repeated practice of targeted exercises, and strategy-based, which involves learning strategies and techniques.
Cognitive training is one particular type of cognitive intervention designed to improve core abilities within targeted domains such as attention, speed of processing (See “Speed of Processing” ), executive function, or memory (See “Cognitive Process” ). There are two major types of cognitive training: process- and strategy-based (Lustig et al. 2009 ). Process-based techniques target improving specific cognitive domains through repeated practice or drills of cognitive exercises. Many different process-based cognitive training programs exist and target domains such as attention, speed of processing,...
This is a preview of subscription content, log in via an institution .
Au J, Sheehan E, Tsai N, Duncan GJ, Buschkuehl M, Jaeggi SM (2015) Improving fluid intelligence with training on working memory: a meta-analysis. Psychon Bull Rev 22(2):366–377. https://doi.org/10.3758/s13423-014-0699-x
Article Google Scholar
Ball KK, Sekuler R (1987) Direction-specific improvement in motion discrimination. Vis Res 27(6):953–965. https://doi.org/10.1016/0042-6989(87)90011-3
Ball KK, Roenker DL, Bruni JR (1990) Developmental changes in attention and visual search throughout adulthood. In: Enns JT (ed) The development of attention: research and theory. Elsevier Science Publishers, Amsterdam, Netherlands, North-Holland, pp 489–595. https://www.sciencedirect.com/science/article/pii/S0166411508604720 , https://doi.org/10.1016/S0166-4115(08)60472-0
Chapter Google Scholar
Ball KK, Berch DB, Helmers KF, Jobe JB, Leveck MD, Marsiske M, … Willis SL (2002) Effects of cognitive training interventions with older adults: a randomized controlled trial. JAMA 288:2271–2281. https://doi.org/10.1001/jama.288.18.2271
Ball KK, Edwards JD, Ross LA, McGwin G Jr (2010) Cognitive training decreases motor vehicle collision involvement of older drivers. J Am Geriatr Soc 58(11):2107–2113. https://doi.org/10.1111/j.1532-5415.2010.03138.x
Brookmeyer R, Johnson E, Ziegler-Graham K, Arrighi HM (2007) Forecasting the global burden of Alzheimer’s disease. Alzheimers Dement 3:181–191. https://doi.org/10.1016/j.jalz.2007.04.381
Edwards JD, Wadley VG, Myers R, Roenker DL, Cissell GM, Ball KK (2002) Transfer of a speed of processing intervention to near and far cognitive functions. Gerontology 48:329–340. https://doi.org/10.1159/000065259
Edwards JD, Wadley VG, Vance DE, Roenker DL, Ball KK (2005) The impact of speed of processing training on cognitive and everyday performance. Aging Ment Health 9:262–271. https://doi.org/10.1080/13607860412331336788
Edwards JD, Delahunt PB, Mahncke HW (2009) Cognitive speed of processing training delays driving cessation. J Gerontol Ser A Biol Sci Med Sci 64:1262–1267. https://doi.org/10.1093/gerona/glp131
Edwards JD, Myers C, Ross LA, Roenker DL, Cissell GM, Mclaughlin A, Ball KK (2009a) The longitudinal impact of speed of processing training on driving mobility of older drivers. Gerontologist 49:485–494. https://doi.org/10.1093/geront/gnp042
Edwards JD, Myers C, Ross LA, Roenker DL, Cissell GM, Mclaughlin A, Ball KK (2009b) The longitudinal impact of speed of processing training upon subsequent mobility of older drivers. Gerontologist 49:485–494. https://doi.org/10.1093/geront/gnp042
Edwards JD, Clark D, Xu H, Guey LT, Ross LA, Unverzagt FW (2017a) Speed of processing training results in lower risk of dementia. Alzheimer’s Dement 3:603–611. https://doi.org/10.1016/j.trci.2017.09.002
Edwards JD, Fausto BA, Tetlow AM, Corona RT, Valdes EG (2017b) Systematic review and meta-analyses of useful field of view cognitive training. Neurosci Biobehav Rev 84:72. https://doi.org/10.1016/j.neubiorev.2017.11.004
Green CS, Bavelier D, Kramer AF, Vinogradov S, Ansorge U, Ball KK, … Witt CM (2019) Improving methodological standards in behavioral interventions for cognitive enhancement. J Cogn Enhanc 3:1–28. https://doi.org/10.1007/s41465-018-0115-y
Hill NTM, Mowszowski D, Naissmith SL, Chadwick VL, Valenzuela M, Lampit A (2017) Computerized cognitive training in older adults with mild cognitive impairment or dementia: a systematic review and meta-analysis. Am J Psychiatry 174(4):329–340. https://doi.org/10.1176/appi.ajp.2016.16030360
Hindin SB, Zelinski EM (2012) Extended practice and aerobic exercise interventions benefit untrained cognitive outcomes in older adults: a meta-analysis. J Am Geriatr Soc 60(1):136–141. https://doi.org/10.1111/j.1532-5415.2011.03761.x
Humes LE, Busey TA, Craig J, Kewley-Port D (2013) Are age-related changes in cognitive function driven by age-related changes in sensory processing? Atten Percept Psychophys 75(3):508–524. https://doi.org/10.3758/s13414-012-0406-9
Institute of Medicine (2015) Cognitive aging: progress in understanding and opportunity for action. National Academies Press, Washington, DC
Google Scholar
Kelly ME, Loughrey D, Lawlor BA, Robertson IH, Walsh C, Brennan S (2014) The impact of cognitive training and mental stimulation on cognitive and everyday functioning of healthy older adults: a systematic review and meta-analysis. Ageing Res Rev 15:28–43. https://doi.org/10.1016/j.arr.2014.02.004
Kueider AM, Parisi JM, Gross AL, Rebok G (2012) Computerized cognitive training with older adults: a systematic review. PLoS One 7(7):e40588. https://doi.org/10.1371/journal.pone.0040588
Lampit A, Hallock H, Valenzuela M (2014) Computerized cognitive training in cognitively healthy older adults: a systematic review and meta-analysis of effect modifiers. PLoS Med 11(11):e1001756. https://doi.org/10.1371/journal.pmed.1001756
Lampit A, Valenzuela M, Gates NJ (2015) Computerized cognitive training is beneficial for older adults. J Am Geriatr Soc 63(12):2610–2612. https://doi.org/10.1111/jgs.13825
Lin F, Heffner KL, Ren P, Tivarus ME, Brasch J, Chen DG, … Tadin D (2016) Cognitive and neural effects of vision-based speed-of-processing training in older adults with amnestic mild cognitive impairment: a pilot study. J Am Geriatr Soc 64(6):1293–1298. https://doi.org/10.1111/jgs.14132
Lustig C, Shah P, Seidler R, Reuter-Lorenz PA (2009) Aging, Training, and the Brain: A Review and Future Directions. Neuropsychol Rev https://doi.org/10.1007/s11065-009-9119-9
Mewborn CM, Lindbergh CA, Miller LS (2017) Cognitive interventions for cognitively healthy, mildly impaired, and mixed samples of older adults: a systematic review and meta-analysis of randomized-controlled trials. [journal article]. Neuropsychol Rev 27(4):403–439. https://doi.org/10.1007/s11065-017-9350-8
National Academies of Sciences, Engineering and Medicine (2017) Preventing cognitive decline and dementia: a way forward. The National Academies Press, Washington, DC
Noack H, Lovden M, Schmiedek F, Lindenberger U (2009) Cognitive plasticity in adulthood and old age: gauging the generality of cognitive intervention effects. Restor Neurol Neurosci 27:435–453. https://doi.org/10.3233/RNN-2009-0496
Park DC, Lodi-Smith J, Drew L, Haber S, Hebrank A, Bischof GN, Aamodt W (2014) The impact of sustained engagement on cognitive function in older adults: the synapse project. Psychol Sci 25(1):103–112. https://doi.org/10.1177/0956797613499592
Rebok GW, Ball K, Guey LT, Jones RN, Kim HY, King JW, … Willis SL (2014) Ten-year effects of the advanced cognitive training for independent and vital elderly cognitive training trial on cognition and everyday functioning in older adults. J Am Geriatr Soc 62(1):16–24. https://doi.org/10.1111/jgs.12607
Reijnders J, Heugten CV, Boxtel MV (2013) Cognitive interventions in healthy older adults and people with mild cognitive impairment: a systematic review. Ageing Res Rev 12:263–275. https://doi.org/10.1016/j.arr.2012.07.003
Roenker DL, Cissell GM, Ball KK, Wadley VG, Edwards JD (2003) Speed-of-processing and driving simulator training result in improved driving performance. Hum Factors 45(2):218–233
Sekuler R, Ball KK (1986) Visual localization: age and practice. J Opt Soc Am A 3(6):864–867
Smith-Ray RL, Hughes SL, Prohaska TR, Little DM, Jurivich DA, Hedeker D (2014) Impact of cognitive training on balance and gait in older adults. J Gerontol Ser A Biol Sci Med Sci 70:357–366. https://doi.org/10.1093/geronb/gbt097
Sprague BN, Freed SA, Webb, CE, Phillips C, Hyun J, Ross LA (2019) The impact of behavioral interventions on cognitive function in healthy older adults: a systematic review. Ageing Research Reviews 52:32–52. https://doi.org/10.1016/j.arr.2019.04.002
Stine-Morrow EAL, Parisi JM, Morrow DG, Park DC (2008) The effects of an engaged lifestyle on cognitive vitality: a field experiment. Psychol Aging 23(4):778–786. https://doi.org/10.1037/a0014341
Tsai N, Buschkuehl M, Kamarsu S, Shah P, Jonides J, Jaeggi SM (2018) (Un)great expectations: the role of placebo effects in cognitive training. J Appl Res Mem Cogn 7(4):564–573. https://doi.org/10.1016/j.jarmac.2018.06.001
Van Vleet TM, DeGutis JM, Merzenich MM, Simpson G, Zomet A, Dabit S (2016) Targeting alertness to improve cognition in older adults: a preliminary report of benefits in executive function and skill acquisition. Cortex 82:100–116
Webb SL, Loh V, Lampit A, Bateman JE, Birney DP (2018) Meta-analysis of the effects of computerized cognitive training on executive functions: a cross-disciplinary taxonomy for classifying outcome cognitive factors. Neuropsychol Rev 28(2):232–250. https://doi.org/10.1159/000323950
Willis SL, Tennstedt SL, Marsiske M, Ball KK, Elias J, Koepke KM, … Wright E (2006) Long-term effects of cognitive training on everyday functional outcomes in older adults. JAMA 296(23):2805–2814. https://doi.org/10.1001/jama.296.23.2805
Wolinsky FD, Unverzagt FW, Smith DM, Jones R, Stoddard A, Tennstetdt SL (2006) The ACTIVE cognitive training trial and health-related quality of life: protection that lasts for 5 years. J Gerontol Ser A Biol Sci Med Sci 61:1324–1329
Wolinsky FD, Mahncke HW, Kosinski M et al (2009a) The ACTIVE cognitive training trial and predicted medical expenditures. BMC Health Serv Res 9(109). https://doi.org/10.1186/1472-6963-9-109
Wolinsky FD, Mahncke HW, Vander Weg MW et al (2009b) The effect of speed-of-processing training on depressive symptoms in ACTIVE. J Gerontol Ser A Biol Sci Med Sci 64A:468–472
Wolinsky FD, Mahncke HW, Vander Weg MW, Martin R, Unverzagt FW, Ball KK, … Tennstedt SL (2010) Speed of processing training protects self-rated health in older adults: enduring effects observed in the multi-site ACTIVE randomized controlled trial. Int Psychogeriatr 22:470–478
Wolinsky FD, Vander Weg MW, Howren MB, Jones MP, Dotson MM (2015) The effect of cognitive speed of processing training on the development of additional IADL difficulties and the reduction of depressive symptoms: results from the IHAMS randomized controlled trial. J Aging Health 27(2):334–354. https://doi.org/10.1177/0898264314550715
Download references
Author information
Authors and affiliations.
Department of Psychiatry and Behavioral Neurosciences, University of South Florida, Tampa, FL, USA
Jerri D. Edwards
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Jerri D. Edwards .
Editor information
Editors and affiliations.
Population Division, UN Dept of Economic Social Affairs Population Division, New York, NY, USA
Department of Population Health Sciences, Duke University School of Medicine, Durham, NC, USA
Matthew E. Dupre
Section Editor information
Center for Cognitive Aging and Memory, Department of Clinical and Health Psychology, McKnight Brain Institute, College of Public Health and Health Professions, University of Florida, Gainesville, FL, USA
Adam J. Woods
Department of Neuroscience, University of Florida, Gainesville, FL, USA
Rights and permissions
Reprints and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this entry
Cite this entry.
Edwards, J.D. (2019). Cognitive Training. In: Gu, D., Dupre, M. (eds) Encyclopedia of Gerontology and Population Aging. Springer, Cham. https://doi.org/10.1007/978-3-319-69892-2_693-1
Download citation
DOI : https://doi.org/10.1007/978-3-319-69892-2_693-1
Received : 22 March 2019
Accepted : 14 June 2019
Published : 01 July 2019
Publisher Name : Springer, Cham
Print ISBN : 978-3-319-69892-2
Online ISBN : 978-3-319-69892-2
eBook Packages : Springer Reference Biomedicine and Life Sciences Reference Module Biomedical and Life Sciences
- Publish with us
Policies and ethics
- Find a journal
- Track your research
Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- Review Article
- Published: 12 January 2022
Mechanisms underlying training-induced cognitive change
- Claudia C. von Bastian ORCID: orcid.org/0000-0002-0667-2460 1 ,
- Sylvie Belleville 2 , 4 ,
- Robert C. Udale 1 ,
- Alice Reinhartz ORCID: orcid.org/0000-0001-6156-9864 3 ,
- Mehdi Essounni 4 &
- Tilo Strobach ORCID: orcid.org/0000-0001-7840-0651 3
Nature Reviews Psychology volume 1 , pages 30–41 ( 2022 ) Cite this article
9769 Accesses
29 Citations
41 Altmetric
Metrics details
- Behavioural methods
- Cognitive control
- Learning and memory
- Working memory
The prospect of enhancing cognition through behavioural training interventions, for example, the repetitive practice of cognitive tasks or metacognitive strategy instruction, has seen a surge in popularity over the past 20 years. Although overwhelming evidence demonstrates that such training interventions increase performance in the trained tasks, controversy remains over whether these benefits transfer to other tasks and abilities beyond the trained context. In this Review, we provide an overview of the effectiveness of cognitive training to induce transfer to untrained tasks, with a particular focus on the theoretical mechanisms that have been proposed to underlie training and transfer effects. We highlight that there is relatively little evidence that training enhances cognitive capacity, that is, the overall cognitive resources available to an individual. By contrast, substantial evidence supports training-induced improvements in cognitive efficiency, that is, optimized performance within existing cognitive capacity limits. We conclude that shifting research towards identifying the cognitive mechanisms underlying gains in cognitive efficiency offers a fruitful avenue for developing effective cognitive training interventions. However, to advance our understanding of human cognition and cognitive plasticity we must strive to develop and refine theories that generate testable hypotheses.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 digital issues and online access to articles
55,14 € per year
only 4,60 € per issue
Rent or buy this article
Prices vary by article type
Prices may be subject to local taxes which are calculated during checkout
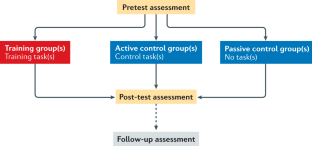
Similar content being viewed by others

A dual-process model for cognitive training
Julia Ericson & Torkel Klingberg

Principles of cognitive control over task focus and task switching
Tobias Egner

Leveraging technology to personalize cognitive enhancement methods in aging
David A. Ziegler, Joaquin A. Anguera, … Adam Gazzaley
Lövdén, M., Bäckman, L., Lindenberger, U., Schaefer, S. & Schmiedek, F. A theoretical framework for the study of adult cognitive plasticity. Psychol. Bull. 136 , 659–676 (2010).
Article Google Scholar
Kühn, S. & Lindenberger, U. in Handbook of the Psychology of Aging 8th edn (eds Schaie, K. W. & Willis, S. L.) 105–123 (Academic, 2016).
Lindenberger, U. & Lövdén, M. Brain plasticity in human lifespan development: the exploration–selection–refinement model. Annu. Rev. Dev. Psychol. 1 , 197–222 (2019).
Baltes, P. B. & Baltes, M. M. in Successful Aging: Perspectives from the Behavioral Sciences (eds Baltes, P. B. & Baltes, M. M.) 1–34 (Cambridge Univ. Press, 1990).
Martinussen, R., Hayden, J., Hogg-Johnson, S. & Tannock, R. A meta-analysis of working memory impairments in children with attention-deficit/hyperactivity disorder. J. Am. Acad. Child. Adolesc. Psychiatry 44 , 377–384 (2005).
Demetriou, E. A. et al. Autism spectrum disorders: a meta-analysis of executive function. Mol. Psychiatry 23 , 1198–1204 (2018).
Arvanitakis, Z., Shah, R. C. & Bennett, D. A. Diagnosis and management of dementia: review. JAMA 322 , 1589–1599 (2019).
Lugtmeijer, S., Lammers, N. A., de Haan, E. H. F., de Leeuw, F.-E. & Kessels, R. P. C. Post-stroke working memory dysfunction: a meta-analysis and systematic review. Neuropsychol. Rev. 31 , 202–219 (2021).
Hommel, B. Pseudo-mechanistic explanations in psychology and cognitive neuroscience. Top. Cogn. Sci. 12 , 1294–1305 (2020).
Simons, D. J. et al. Do “brain-training” programs work? Psychol. Sci. Public. Interest. 17 , 103–186 (2016).
Sala, G. et al. Near and far transfer in cognitive training: a second-order meta-analysis. Collabra: Psychol. 5 , 18 (2019).
Sala, G. & Gobet, F. Cognitive training does not enhance general cognition. Trends Cogn. Sci. 23 , 9–20 (2019).
Borella, E., Carretti, B., Riboldi, F. & De Beni, R. Working memory training in older adults: evidence of transfer and maintenance effects. Psychol. Aging 25 , 767–778 (2010).
Schmiedek, F., Lövdén, M. & Lindenberger, U. Hundred days of cognitive training enhance broad cognitive abilities in adulthood: findings from the COGITO study. Front. Aging Neurosci. 2 , 27 (2010).
Google Scholar
Barnett, S. M. & Ceci, S. J. When and where do we apply what we learn? A taxonomy for far transfer. Psychol. Bull. 128 , 612–637 (2002).
Noack, H., Lövdén, M., Schmiedek, F. & Lindenberger, U. Cognitive plasticity in adulthood and old age: gauging the generality of cognitive intervention effects. Restor. Neurol. Neurosci. 27 , 435–453 (2009).
Foroughi, C. K., Monfort, S. S., Paczynski, M., McKnight, P. E. & Greenwood, P. M. Placebo effects in cognitive training. Proc. Natl Acad. Sci. USA 113 , 7470 (2016).
Boot, W. R., Simons, D. J., Stothart, C. & Stutts, C. The pervasive problem with placebos in psychology: why active control groups are not sufficient to rule out placebo effects. Perspect. Psychol. Sci. 8 , 445–454 (2013).
von Bastian, C. C. & Oberauer, K. Effects and mechanisms of working memory training: a review. Psychol. Res. 78 , 803–820 (2014).
Green, C. S. et al. Improving methodological standards in behavioral interventions for cognitive enhancement. J. Cogn. Enhanc. 3 , 2–29 (2019).
Green, C. S., Strobach, T. & Schubert, T. On methodological standards in training and transfer experiments. Psychol. Res. 78 , 756–772 (2014).
Dahlin, E., Neely, A. S., Larsson, A., Bäckman, L. & Nyberg, L. Transfer of learning after updating training mediated by the striatum. Science 320 , 1510–1512 (2008).
Anguera, J. A. et al. Video game training enhances cognitive control in older adults. Nature 501 , 97–101 (2013).
Rebok, G. W. et al. Ten-year effects of the Advanced Cognitive Training for Independent and Vital Elderly cognitive training trial on cognition and everyday functioning in older adults. J. Am. Geriatr. Soc. 62 , 16–24 (2014).
Motter, J. N., Grinberg, A., Lieberman, D. H., Iqnaibi, W. B. & Sneed, J. R. Computerized cognitive training in young adults with depressive symptoms: effects on mood, cognition, and everyday functioning. J. Affect. Disord. 245 , 28–37 (2019).
Shipstead, Z., Redick, T. S. & Engle, R. W. Is working memory training effective? Psychol. Bull. 138 , 628–654 (2012).
Hicks, K. & Engle, R. W. in Cognitive and Working Memory Training: Perspectives from Psychology, Neuroscience, and Human Development (eds Bunting, M. F., Novick, J. M., Dougherty, M. R., & Engle, R. W.) 3–13 (Oxford Univ. Press, 2019).
Miyake, A. et al. The unity and diversity of executive functions and their contributions to complex “frontal lobe” tasks: a latent variable analysis. Cogn. Psychol. 41 , 49–100 (2000).
von Bastian, C. C., Guye, S. & De Simoni, C. in Cognitive and Working Memory Training: Perspectives from Psychology, Neuroscience, and Human Development (eds Bunting, M. F., Novick, J. M., Dougherty, M. R., & Engle, R. W.) 58–78 (Oxford Univ. Press, 2020).
Lampit, A., Hallock, H. & Valenzuela, M. Computerized cognitive training in cognitively healthy older adults: a systematic review and meta-analysis of effect modifiers. PLoS Med. 11 , e1001756 (2014).
Melby-Lervåg, M., Redick, T. S. & Hulme, C. Working memory training does not improve performance on measures of intelligence or other measures of “far transfer”: evidence from a meta-analytic review. Perspect. Psychol. Sci. 11 , 512–534 (2016).
Hartgerink, C. H. J., Wicherts, J. M. & van Assen, M. A. L. M. Too good to be false: nonsignificant results revisited. Collabra: Psychol. 3 , 9 (2017).
Button, K. S. et al. Power failure: why small sample size undermines the reliability of neuroscience. Nat. Rev. Neurosci. 14 , 365–376 (2013).
Ioannidis, J. P. A. Why most published research findings are false. PLoS Med. 2 , e124 (2005).
Halsey, L. G., Curran-Everett, D., Vowler, S. L. & Drummond, G. B. The fickle P value generates irreproducible results. Nat. Methods 12 , 179–185 (2015).
Valentine, J. C. in The Handbook of Research Synthesis and Meta-Analysis (eds Cooper, H., Hedges, L. V., & Valentine, J. C.) (Russell Sage Foundation, 2009).
Gathercole, S. E., Dunning, D. L., Holmes, J. & Norris, D. Working memory training involves learning new skills. J. Mem. Lang. 105 , 19–42 (2019).
Guye, S., De Simoni, C. & von Bastian, C. C. Do individual differences predict change in cognitive training performance? A latent growth curve modeling approach. J. Cogn. Enhanc. 1 , 374–393 (2017).
Wiemers, E. A., Redick, T. S. & Morrison, A. B. The influence of individual differences in cognitive ability on working memory training gains. J. Cogn. Enhanc. 3 , 174–185 (2019).
Bürki, C. N., Ludwig, C., Chicherio, C. & de Ribaupierre, A. Individual differences in cognitive plasticity: an investigation of training curves in younger and older adults. Psychol. Res. 78 , 821–835 (2014).
Karbach, J., Könen, T. & Spengler, M. Who benefits the most? Individual differences in the transfer of executive control training across the lifespan. J. Cogn. Enhanc. 1 , 394–405 (2017).
Hering, A., Meuleman, B., Bürki, C., Borella, E. & Kliegel, M. Improving older adults’ working memory: the influence of age and crystallized intelligence on training outcomes. J. Cogn. Enhanc. 1 , 358–373 (2017).
Blacker, K. J., Negoita, S., Ewen, J. B. & Courtney, S. M. N -back versus complex span working memory training. J. Cogn. Enhanc. 1 , 434–454 (2017).
von Bastian, C. C. & Eschen, A. Does working memory training have to be adaptive? Psychol. Res. 80 , 181–194 (2016).
Park, D. C. & Bischof, G. N. The aging mind: neuroplasticity in response to cognitive training. Dialogues Clin. Neurosci. 15 , 109–119 (2013).
ten Brinke, L. F., Davis, J. C., Barha, C. K. & Liu-Ambrose, T. Effects of computerized cognitive training on neuroimaging outcomes in older adults: a systematic review. BMC Geriatr. 17 , 139 (2017).
Brehmer, Y. et al. Neural correlates of training-related working-memory gains in old age. Neuroimage 58 , 1110–1120 (2011).
Thorndike, E. L. & Woodworth, R. S. The influence of improvement in one mental function upon the efficiency of other functions. Psychol. Rev. 8 , 247–261 (1901).
Taatgen, N. A. The nature and transfer of cognitive skills. Psychol. Rev. 120 , 439–471 (2013).
Carroll, J. B. Human Cognitive Abilities: A Survey of Factor-Analytic Studies (Cambridge Univ. Press, 1993).
Zimmermann, K., von Bastian, C. C., Röcke, C., Martin, M. & Eschen, A. Transfer after process-based object-location memory training in healthy older adults. Psychol. Aging 31 , 798–814 (2016).
Garlick, D. Understanding the nature of the general factor of intelligence: the role of individual differences in neural plasticity as an explanatory mechanism. Psychol. Rev. 109 , 116–136 (2002).
De Simoni, C. & von Bastian, C. C. Working memory updating and binding training: Bayesian evidence supporting the absence of transfer. J. Exp. Psychol. Gen. 147 , 829–858 (2018).
Meiran, N., Dreisbach, G. & von Bastian, C. C. Mechanisms of working memory training: insights from individual differences. Intelligence 73 , 78–87 (2019).
Chein, J. M. & Schneider, W. The brain’s learning and control architecture. Curr. Dir. Psychol. Sci. 21 , 78–84 (2012).
Taatgen, N. A. in Cognitive training: An Overview of Features and Applications (eds Strobach, T. & Karbach, J.) 41–54 (Springer, 2021).
Edwards, J. D., Fausto, B. A., Tetlow, A. M., Corona, R. T. & Valdés, E. G. Systematic review and meta-analyses of useful field of view cognitive training. Neurosci. Biobehav. Rev. 84 , 72–91 (2018).
Cásedas, L., Pirrucio, V., Vadillo, M. A. & Lupiáñez, J. Does mindfulness meditation training enhance executive control? A systematic review and meta-analysis of randomized controlled trials in adults. Mindfulness 11 , 411–424 (2020).
Verhaeghen, P. Mindfulness as attention training: meta-analyses on the links between attention performance and mindfulness interventions, long-term meditation practice, and trait mindfulness. Mindfulness 12 , 564–581 (2021).
Gill, L.-N., Renault, R., Campbell, E., Rainville, P. & Khoury, B. Mindfulness induction and cognition: a systematic review and meta-analysis. Conscious. Cogn. 84 , 102991 (2020).
Green, C. S. & Bavelier, D. Action video game training for cognitive enhancement. Curr. Opin. Behav. Sci. 4 , 103–108 (2015).
Bediou, B. et al. Meta-analysis of action video game impact on perceptual, attentional, and cognitive skills. Psychol. Bull. 144 , 77–110 (2018).
Ball, K. & Owsley, C. The useful field of view test: a new technique for evaluating age-related declines in visual function. J. Am. Optom. Assoc. 64 , 71–79 (1993).
Wood, J. M. & Owsley, C. Useful field of view test. Gerontology 60 , 315–318 (2014).
Benikos, N., Johnstone, S. J. & Roodenrys, S. J. Short-term training in the go/nogo task: behavioural and neural changes depend on task demands. Int. J. Psychophysiol. 87 , 301–312 (2013).
Zhao, X., Chen, L. & Maes, J. H. R. Training and transfer effects of response inhibition training in children and adults. Dev. Sci. 21 , e12511 (2018).
Hartmann, L., Sallard, E. & Spierer, L. Enhancing frontal top-down inhibitory control with go/nogo training. Brain Struct. Funct. 221 , 3835–3842 (2016).
Maraver, M. J., Bajo, M. T. & Gomez-Ariza, C. J. Training on working memory and inhibitory control in young adults. Front. Hum. Neurosci. 10 , 588 (2016).
Berkman, E. T., Kahn, L. E. & Merchant, J. S. Training-induced changes in inhibitory control network activity. J. Neurosci. 34 , 149 (2014).
Strobach, T., Salminen, T., Karbach, J. & Schubert, T. Practice-related optimization and transfer of executive functions: a general review and a specific realization of their mechanisms in dual tasks. Psychol. Res. 78 , 836–851 (2014).
Allom, V., Mullan, B. & Hagger, M. Does inhibitory control training improve health behaviour? A meta-analysis. Health Psychol. Rev. 10 , 168–186 (2016).
Jones, A., Tiplady, B., Houben, K., Nederkoorn, C. & Field, M. Do daily fluctuations in inhibitory control predict alcohol consumption? An ecological momentary assessment study. Psychopharmacology 235 , 1487–1496 (2018).
Houben, K. & Jansen, A. Training inhibitory control. A recipe for resisting sweet temptations. Appetite 56 , 345–349 (2011).
Strobach, T. & Schubert, T. in Cognitive Training (eds Strobach, T. & Karbach, J.) 229–241 (Springer, 2021).
Sala, G., Tatlidil, K. S. & Gobet, F. Video game training does not enhance cognitive ability: a comprehensive meta-analytic investigation. Psychol. Bull. 144 , 111–139 (2018).
Hilgard, J., Sala, G., Boot, W. R. & Simons, D. J. Overestimation of action-game training effects: publication bias and salami slicing. Collabra: Psychol. 5 , 30 (2019).
Bavelier, D., Green, C. S., Pouget, A. & Schrater, P. Brain plasticity through the life span: learning to learn and action video games. Annu. Rev. Neurosci. 35 , 391–416 (2012).
Kattner, F., Cochrane, A., Cox, C. R., Gorman, T. E. & Green, C. S. Perceptual learning generalization from sequential perceptual training as a change in learning rate. Curr. Biol. 27 , 840–846 (2017).
Kemp, C., Goodman, N. D. & Tenenbaum, J. B. Learning to learn causal models. Cogn. Sci. 34 , 1185–1243 (2010).
Barrett, L. F., Tugade, M. M. & Engle, R. W. Individual differences in working memory capacity and dual-process theories of the mind. Psychol. Bull. 130 , 553–573 (2004).
Klingberg, T. Training and plasticity of working memory. Trends Cogn. Sci. 14 , 317–324 (2010).
Jaeggi, S. M., Buschkuehl, M., Jonides, J. & Perrig, W. J. Improving fluid intelligence with training on working memory. Proc. Natl Acad. Sci. USA 105 , 6829 (2008).
Klingberg, T. et al. Computerized training of working memory in children with ADHD — a randomized, controlled trial. J. Am. Acad. Child. Adolesc. Psychiatry 44 , 177–186 (2005).
Redick, T. S. et al. No evidence of intelligence improvement after working memory training: a randomized, placebo-controlled study. J. Exp. Psychol. Gen. 142 , 359 (2013).
Chein, J. M. & Morrison, A. B. Expanding the mind’s workspace: training and transfer effects with a complex working memory span task. Psychon. Bull. Rev. 17 , 193–199 (2010).
Guye, S. & von Bastian, C. C. Working memory training in older adults: Bayesian evidence supporting the absence of transfer. Psychol. Aging 32 , 732–746 (2017).
Sprenger, A. M. et al. Training working memory: limits of transfer. Intelligence 41 , 638–663 (2013).
Au, J. et al. Improving fluid intelligence with training on working memory: a meta-analysis. Psychon. Bull. Rev. 22 , 366–377 (2015).
Karbach, J. & Verhaeghen, P. Making working memory work: a meta-analysis of executive-control and working memory training in older adults. Psychol. Sci. 25 , 2027–2037 (2014).
Schwaighofer, M., Fischer, F. & Bühner, M. Does working memory training transfer? A meta-analysis including training conditions as moderators. Educ. Psychol. 50 , 138–166 (2015).
Soveri, A., Antfolk, J., Karlsson, L., Salo, B. & Laine, M. Working memory training revisited: a multi-level meta-analysis of n -back training studies. Psychon. Bull. Rev. 24 , 1077–1096 (2017).
Sala, G. & Gobet, F. Working memory training in typically developing children: a multilevel meta-analysis. Psychon. Bull. Rev. 27 , 423–434 (2020).
Sala, G., Aksayli, N. D., Tatlidil, K. S., Gondo, Y. & Gobet, F. Working memory training does not enhance older adults’ cognitive skills: a comprehensive meta-analysis. Intelligence 77 , 101386 (2019).
Langer, N., von Bastian, C. C., Wirz, H., Oberauer, K. & Jäncke, L. The effects of working memory training on functional brain network efficiency. Cortex 49 , 2424–2438 (2013).
Dziemian, S., Appenzeller, S., von Bastian, C. C., Jäncke, L. & Langer, N. Working memory training effects on white matter integrity in young and older adults. Front. Hum. Neurosci. 15 , 605213 (2021).
Lawlor-Savage, L., Clark, C. M. & Goghari, V. M. No evidence that working memory training alters gray matter structure: a MRI surface-based analysis. Behav. Brain Res. 360 , 323–340 (2019).
Laine, M., Fellman, D., Waris, O. & Nyman, T. J. The early effects of external and internal strategies on working memory updating training. Sci. Rep. 8 , 4045 (2018).
Dunning, D. L. & Holmes, J. Does working memory training promote the use of strategies on untrained working memory tasks? Mem. Cognit. 42 , 854–862 (2014).
Chase, W. G. & Ericsson, K. A. in Cognitive Skills and Their Acquisition (ed. Anderson, J. R.) 141–189 (Erlbaum, 1981).
Redick, T. S., Wiemers, E. A. & Engle, R. W. The role of proactive interference in working memory training and transfer. Psychol. Res. 84 , 1635–1654 (2020).
Zerr, P. et al. The development of retro-cue benefits with extensive practice: implications for capacity estimation and attentional states in visual working memory. Mem. Cognit. 49 , 1036–1049 (2021).
Brady, T. F., Konkle, T. & Alvarez, G. A. Compression in visual working memory: using statistical regularities to form more efficient memory representations. J. Exp. Psychol. Gen. 138 , 487–502 (2009).
Verhaeghen, P., Marcoen, A. & Goossens, L. Improving memory performance in the aged through mnemonic training: a meta-analytic study. Psychol. Aging 7 , 242–251 (1992).
Ball, K. et al. Effects of cognitive training interventions with older adults: a randomized controlled trial. JAMA 288 , 2271–2281 (2002).
Belleville, S. et al. Improvement of episodic memory in persons with mild cognitive impairment and healthy older adults: evidence from a cognitive intervention program. Dement. Geriatr. Cogn. Disord. 22 , 486–499 (2006).
Belleville, S. et al. MEMO+: efficacy, durability and effect of cognitive training and psychosocial intervention in individuals with mild cognitive impairment. J. Am. Geriatr. Soc. 66 , 655–663 (2018).
Hampstead, B. M., Stringer, A. Y., Stilla, R. F., Giddens, M. & Sathian, K. Mnemonic strategy training partially restores hippocampal activity in patients with mild cognitive impairment. Hippocampus 22 , 1652–1658 (2012).
Chandler, M. J., Parks, A. C., Marsiske, M., Rotblatt, L. J. & Smith, G. E. Everyday impact of cognitive interventions in mild cognitive impairment: a systematic review and meta-analysis. Neuropsychol. Rev. 26 , 225–251 (2016).
Bottiroli, S., Cavallini, E., Dunlosky, J., Vecchi, T. & Hertzog, C. The importance of training strategy adaptation: a learner-oriented approach for improving older adults’ memory and transfer. J. Exp. Psychol. Appl. 19 , 205–218 (2013).
Bellander, M. et al. No evidence for improved associative memory performance following process-based associative memory training in older adults. Front. Aging Neurosci. 8 , 326 (2017).
Glenberg, A. M. & Lehmann, T. S. Spacing repetitions over 1 week. Mem. Cognit. 8 , 528–538 (1980).
Bjork, R. A. in Practical Aspects of Memory: Current Research and Issues, Vol. 1: Memory in Everyday Life (eds Gruneberg, M. M., Morris, P. E. & Sykes, R. N.) 396–401 (Wiley, 1988).
Logan, J. M. & Balota, D. A. Expanded vs. equal interval spaced retrieval practice: exploring different schedules of spacing and retention interval in younger and older adults. Aging Neuropsychol. Cogn. 15 , 257–280 (2008).
Karpicke, J. D. & Bauernschmidt, A. Spaced retrieval: absolute spacing enhances learning regardless of relative spacing. J. Exp. Psychol. Learn. Mem. Cogn. 37 , 1250–1257 (2011).
Jennings, J. M. & Jacoby, L. L. Improving memory in older adults: training recollection. Neuropsychol. Rehabil. 13 , 417–440 (2003).
Jennings, J. M., Webster, L. M., Kleykamp, B. A. & Dagenbach, D. Recollection training and transfer effects in older adults: successful use of a repetition-lag procedure. Aging Neuropsychol. Cogn. 12 , 278–298 (2005).
Anderson, N. D., Ebert, P. L., Grady, C. L. & Jennings, J. M. Repetition lag training eliminates age-related recollection deficits (and gains are maintained after three months) but does not transfer: implications for the fractionation of recollection. Psychol. Aging 33 , 93–108 (2018).
Boller, B., Jennings, J. M., Dieudonné, B., Verny, M. & Ergis, A.-M. Recollection training and transfer effects in Alzheimer’s disease: effectiveness of the repetition-lag procedure. Brain Cogn. 78 , 169–177 (2012).
Jennings, J. M., Lopina, E. C. & Dagenbach, D. in Remembering (eds Lindsay, D. S., Kelley, C. M., Yonelinas, A. P. & Roediger III, H. L) 276–292 (Psychology, 2014).
Stamenova, V. et al. Training recollection in healthy older adults: clear improvements on the training task, but little evidence of transfer. Front. Hum. Neurosci. 8 , 898 (2014).
Bailey, H., Dagenbach, D. & Jennings, J. M. The locus of the benefits of repetition-lag memory training. Aging Neuropsychol. Cogn. 18 , 577–593 (2011).
Koch, I., Poljac, E., Müller, H. & Kiesel, A. Cognitive structure, flexibility, and plasticity in human multitasking — an integrative review of dual-task and task-switching research. Psychol. Bull. 144 , 557–583 (2018).
Nguyen, L., Murphy, K. & Andrews, G. Immediate and long-term efficacy of executive functions cognitive training in older adults: a systematic review and meta-analysis. Psychol. Bull. 145 , 698–733 (2019).
Dörrenbächer, S. & Kray, J. The impact of game-based task-shifting training on motivation and executive control in children with ADHD. J. Cogn. Enhanc. 3 , 64–84 (2019).
Minear, M. & Shah, P. Training and transfer effects in task switching. Mem. Cognit. 36 , 1470–1483 (2008).
Karbach, J. & Kray, J. How useful is executive control training? Age differences in near and far transfer of task-switching training. Dev. Sci. 12 , 978–990 (2009).
von Bastian, C. C. & Oberauer, K. Distinct transfer effects of training different facets of working memory capacity. J. Mem. Lang. 69 , 36–58 (2013).
Pereg, M., Shahar, N. & Meiran, N. Task switching training effects are mediated by working-memory management. Intelligence 41 , 467–478 (2013).
Zinke, K., Zeintl, M., Eschen, A., Herzog, C. & Kliegel, M. Potentials and limits of plasticity induced by working memory training in old-old age. Gerontology 58 , 79–87 (2012).
Braver, T. S. The variable nature of cognitive control: a dual mechanisms framework. Trends Cogn. Sci. 16 , 106–113 (2012).
Schumacher, E. H. et al. Virtually perfect time sharing in dual-task performance: uncorking the central cognitive bottleneck. Psychol. Sci. 12 , 101–108 (2001).
Schubert, T. & Strobach, T. Practice-related optimization of dual-task performance: efficient task instantiation during overlapping task processing. J. Exp. Psychol. Hum. Percept. Perform. 44 , 1884–1904 (2018).
Bier, B., de Boysson, C. & Belleville, S. Identifying training modalities to improve multitasking in older adults. Age 36 , 9688 (2014).
Gagnon, L. G. & Belleville, S. Training of attentional control in mild cognitive impairment with executive deficits: results from a double-blind randomised controlled study. Neuropsychol. Rehabil. 22 , 809–835 (2012).
Lee, H. et al. Performance gains from directed training do not transfer to untrained tasks. Acta Psychol. 139 , 146–158 (2012).
Voss, M. W. et al. Effects of training strategies implemented in a complex videogame on functional connectivity of attentional networks. Neuroimage 59 , 138–148 (2012).
Bherer, L. et al. Testing the limits of cognitive plasticity in older adults: application to attentional control. Acta Psychol. 123 , 261–278 (2006).
Bherer, L. et al. Training effects on dual-task performance: are there age-related differences in plasticity of attentional control? Psychol. Aging 20 , 695–709 (2005).
Kramer, A. F., Larish, J. F. & Strayer, D. L. Training for attentional control in dual task settings: a comparison of young and old adults. J. Exp. Psychol. Appl. 1 , 50–76 (1995).
Hazeltine, E., Teague, D. & Ivry, R. B. Simultaneous dual-task performance reveals parallel response selection after practice. J. Exp. Psychol. Hum. Percept. Perform. 28 , 527–545 (2002).
Liepelt, R., Strobach, T., Frensch, P. & Schubert, T. Improved intertask coordination after extensive dual-task practice. Q. J. Exp. Psychol. 64 , 1251–1272 (2011).
Strobach, T., Frensch, P., Müller, H. & Schubert, T. Evidence for the acquisition of dual-task coordination skills in older adults. Acta Psychol. 160 , 104–116 (2015).
Strobach, T., Frensch, P. A. & Schubert, T. Video game practice optimizes executive control skills in dual-task and task switching situations. Acta Psychol. 140 , 13–24 (2012).
Strobach, T., Frensch, P. A., Soutschek, A. & Schubert, T. Investigation on the improvement and transfer of dual-task coordination skills. Psychol. Res. 76 , 794–811 (2012).
Bender, A. D., Filmer, H. L., Naughtin, C. K. & Dux, P. E. Dynamic, continuous multitasking training leads to task-specific improvements but does not transfer across action selection tasks. NPJ Sci. Learn. 2 , 14 (2017).
Jensen, A. How much can we boost IQ and scholastic achievement? Harv. Educ. Rev. 39 , 1–123 (1969).
Klingberg, T., Forssberg, H. & Westerberg, H. Training of working memory in children with ADHD. J. Clin. Exp. Neuropsychol. 24 , 781–791 (2002).
Jones, J. S., Milton, F., Mostazir, M. & Adlam, A. R. The academic outcomes of working memory and metacognitive strategy training in children: a double-blind randomized controlled trial. Dev. Sci. 23 , e12870 (2018).
Carpenter, J. et al. Domain-general enhancements of metacognitive ability through adaptive training. J. Exp. Psychol. Gen. 148 , 51–64 (2019).
Belleville, S., Mellah, S., de Boysson, C., Demonet, J.-F. & Bier, B. The pattern and loci of training-induced brain changes in healthy older adults are predicted by the nature of the intervention. PLoS ONE 9 , e102710 (2014).
Boyke, J., Driemeyer, J., Gaser, C., Büchel, C. & May, A. Training-induced brain structure changes in the elderly. J. Neurosci. 28 , 7031 (2008).
Engvig, A. et al. Memory training impacts short-term changes in aging white matter: a longitudinal diffusion tensor imaging study. Hum. Brain Mapp. 33 , 2390–2406 (2012).
Cabeza, R. et al. Maintenance, reserve and compensation: the cognitive neuroscience of healthy ageing. Nat. Rev. Neurosci. 19 , 701–710 (2018).
Stern, Y. et al. Whitepaper: defining and investigating cognitive reserve, brain reserve, and brain maintenance. Alzheimers Dement. 16 , 1305–1311 (2020).
Belleville, S. et al. Training-related brain plasticity in subjects at risk of developing Alzheimer’s disease. Brain 134 , 1623–1634 (2011).
Belleville, S. & Bherer, L. Biomarkers of cognitive training effects in aging. Curr. Transl Geriatr. Exp. Gerontol. Rep. 1 , 104–110 (2012).
Erickson, K. I. et al. Striatal volume predicts level of video game skill acquisition. Cereb. Cortex 20 , 2522–2530 (2010).
Keysers, C., Gazzola, V. & Wagenmakers, E.-J. Using Bayes factor hypothesis testing in neuroscience to establish evidence of absence. Nat. Neurosci. 23 , 788–799 (2020).
Rouder, J. N., Morey, R. D., Verhagen, J., Province, J. M. & Wagenmakers, E.-J. Is there a free lunch in inference? Top. Cogn. Sci. 8 , 520–547 (2016).
Cumming, G. Understanding The New Statistics: Effect Sizes, Confidence Intervals, and Meta-Analysis (Routledge, 2011).
Dienes, Z. Bayesian versus orthodox statistics: which side are you on? Perspect. Psychol. Sci. 6 , 274–290 (2011).
Simmons, J. P., Nelson, L. D. & Simonsohn, U. False-positive psychology: undisclosed flexibility in data collection and analysis allows presenting anything as significant. Psychol. Sci. 22 , 1359–1366 (2011).
Jeffreys, H. The Theory of Probability 3rd edn (Oxford Univ. Press, 1998).
Kass, R. E. & Raftery, A. E. Bayes factors. J. Am. Stat. Assoc. 90 , 773–795 (1995).
Kruschke, J. K. Doing Bayesian Data Analysis: A Tutorial with R and BUGS (Elsevier Academic, 2011).
JASP Team. A fresh way to do statistics. JASP https://jasp-stats.org/ (2018).
Dougherty, M. R., Hamovitz, T. & Tidwell, J. W. Reevaluating the effectiveness of n -back training on transfer through the Bayesian lens: support for the null. Psychon. Bull. Rev. 23 , 306–316 (2016).
Farrell, S. & Lewandowsky, S. Computational Modeling of Cognition and Behavior (Cambridge Univ. Press, 2018).
Redick, T. S. & Lindsey, D. R. B. Complex span and n -back measures of working memory: a meta-analysis. Psychon. Bull. Rev. 20 , 1102–1113 (2013).
Anderson, J. R. How Can The Human Mind Occur In The Physical Universe? (Oxford Univ. Press, 2009).
Takeuchi, H. & Kawashima, R. Effects of processing speed training on cognitive functions and neural systems. Rev. Neurosci. 23 , 289–301 (2012).
Ratcliff, R. A theory of memory retrieval. Psychol. Rev. 85 , 59–108 (1978).
Schmiedek, F., Oberauer, K., Wilhelm, O., Süß, H.-M. & Wittmann, W. W. Individual differences in components of reaction time distributions and their relations to working memory and intelligence. J. Exp. Psychol. Gen. 136 , 414–429 (2007).
van Ravenzwaaij, D., Brown, S. & Wagenmakers, E.-J. An integrated perspective on the relation between response speed and intelligence. Cognition 119 , 381–393 (2011).
Download references
Acknowledgements
The authors acknowledge the support of the Economic and Social Research Council (UK) to C.C.v.B. (ES/V013610/1), the Social Sciences and Humanities Research Council (Canada) to S.B. (2004-2020-0009) and the German Research Foundation to T.S. (STR 1223/10-1).
Author information
Authors and affiliations.
Department of Psychology, University of Sheffield, Sheffield, UK
Claudia C. von Bastian & Robert C. Udale
Department of Psychology, Université de Montréal, Montreal, Quebec, Canada
Sylvie Belleville
Department of Psychology, Medical School Hamburg, Hamburg, Germany
Alice Reinhartz & Tilo Strobach
Research Center, Institut Universitaire de Gériatrie de Montréal, Montreal, Quebec, Canada
Sylvie Belleville & Mehdi Essounni
You can also search for this author in PubMed Google Scholar
Contributions
All authors researched data for the article. C.C.v.B., S.B. and T.S. contributed substantially to discussion of the content. All authors wrote the article. All authors reviewed and/or edited the manuscript before submission.
Corresponding author
Correspondence to Claudia C. von Bastian .
Ethics declarations
Competing interests.
The authors declare no competing interests.
Additional information
Peer review information.
Nature Reviews Psychology thanks M. Lövdén, R. Maes and G. Sala for their contribution to the peer review of this work.
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Positive training effects in ecologically valid, real-world settings with little experimental control and non-homogeneous samples.
Theoretical constructs specifying the function and organization of one or more cognitive processes and their interplay with other processes and/or biological substrates.
Playing video games with a fast-paced, complex and dynamic visual environment with a high degree of visual clutter and distraction, demanding focused and distributed attention.
Repetitive practice of tasks that are assumed to require basic cognitive processes.
Computer-based measure of the ability to discriminate stimuli presented in central vision with or without concurrent tasks and distractors in peripheral vision.
Computing the probability of one or more random variables using a specific value or set of values.
Quantity of information that can be held accessible in working memory in the present moment.
Ability to solve novel reasoning problems.
Instruction on mental processes or strategies that differ from those typically involved in the task.
One’s belief in their ability to manage and succeed in a particular situation.
Repeated exposures to learning are spread out over time; for example, short practice sessions spread over multiple days.
Repeated exposures to learning are grouped together; for example, one long practice session on a single day.
Differences in performance between repetition trials, in which participants perform the same task as in the previous trial, and switch trials, in which participants perform a different task than in the previous trial.
Differences in performance between dual-task trials, in which participants perform two tasks simultaneously, and single-task trials, in which participants complete one of the two tasks.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Reprints and permissions
About this article
Cite this article.
von Bastian, C.C., Belleville, S., Udale, R.C. et al. Mechanisms underlying training-induced cognitive change. Nat Rev Psychol 1 , 30–41 (2022). https://doi.org/10.1038/s44159-021-00001-3
Download citation
Accepted : 14 September 2021
Published : 12 January 2022
Issue Date : January 2022
DOI : https://doi.org/10.1038/s44159-021-00001-3
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
This article is cited by
Action video games normalise the phonemic awareness in pre-readers at risk for developmental dyslexia.
- Sara Bertoni
- Chiara Andreola
- Andrea Facoetti
npj Science of Learning (2024)
N-Back training in middle adulthood: evidence for transfer only to structurally similar task
- Marija Klara Sedlar
- Andrea Vranic
Current Psychology (2024)
Parental education, cognition and functional connectivity of the salience network
- Pavla Cermakova
- Adam Chlapečka
- Klára Marečková
Scientific Reports (2023)
Efficiency and capacity mechanisms can coexist in cognitive training
- Da-Wei Zhang
- Bruno Sauce
Nature Reviews Psychology (2023)
The relationship between bilingual language use and executive functions
- Minna Lehtonen
- Valantis Fyndanis
- Jussi Jylkkä
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies
Sign up for the Nature Briefing newsletter — what matters in science, free to your inbox daily.

IMAGES
VIDEO
COMMENTS
Key points. Problem-solving is one technique used on the behavioral side of cognitive-behavioral therapy. The problem-solving technique is an iterative, five-step process that requires one to ...
High-order memory and problem-solving skills (including executive functioning and verbal skills) This technique assumes a degree of neuroplasticity that, with training, results in a greater degree of accuracy in sensory representations, improved cognitive strategies for grouping stimuli into more meaningful groups, and better recall.
“Problem-solving therapy (PST) is a psychosocial intervention, generally considered to be under a cognitive-behavioral umbrella” (Nezu, Nezu, & D’Zurilla, 2013, p. ix). It aims to encourage the client to cope better with day-to-day problems and traumatic events and reduce their impact on mental and physical wellbeing.
perception. mental rotation. working memory. reasoning. The study concluded that doing jigsaw puzzles regularly and throughout life may protect against the effects of brain aging. 7. Playing ...
Cognitive training is an approach that seeks to sharpen or maintain brain functions through the use of regular mental activities. These mental activities are intended to help cognitive abilities such as working memory, executive function, and problem-solving abilities. There is a long-standing notion that playing brain games, such as puzzles ...
Cognitive skills related to information-processing and problem-solving: Direction and Orientation: These skills make it easier to understand relationships in the environment. They allow you to give, take, and prioritize directions. Classification and Categorization: These skills allow you to group and reorganize ideas, emotions, objects ...
The cognitive training tasks each target a particular core cognitive ability and are grouped into five categories by target domain: speed of processing, attention, memory, flexibility, and problem solving.
Strategy-based cognitive training focuses on learning and practicing strategies (e.g., mnemonics for memory) to improve a domain of cognitive function such as reasoning, problem solving, or memory. For older adults, cognitive training is typically designed for those with age-related cognitive decline or mild cognitive impairment (See “Mild ...
Cognitive training interventions typically target cognitive abilities that are central to human learning, problem-solving and innovation throughout the lifespan, including the basic abilities ...
You can find dual n-back exercises online on various websites and apps dedicated to brain training. 6. Crossword puzzles. Crossword puzzles are word games that require you to fill in a grid with ...